Mistakes are an inherent learning opportunity within healthcare that can be used to prevent future loss of lives and reduce suffering. We aim to create a safe learning space within our organization that can be embedded within our quality improvement (QI) process.
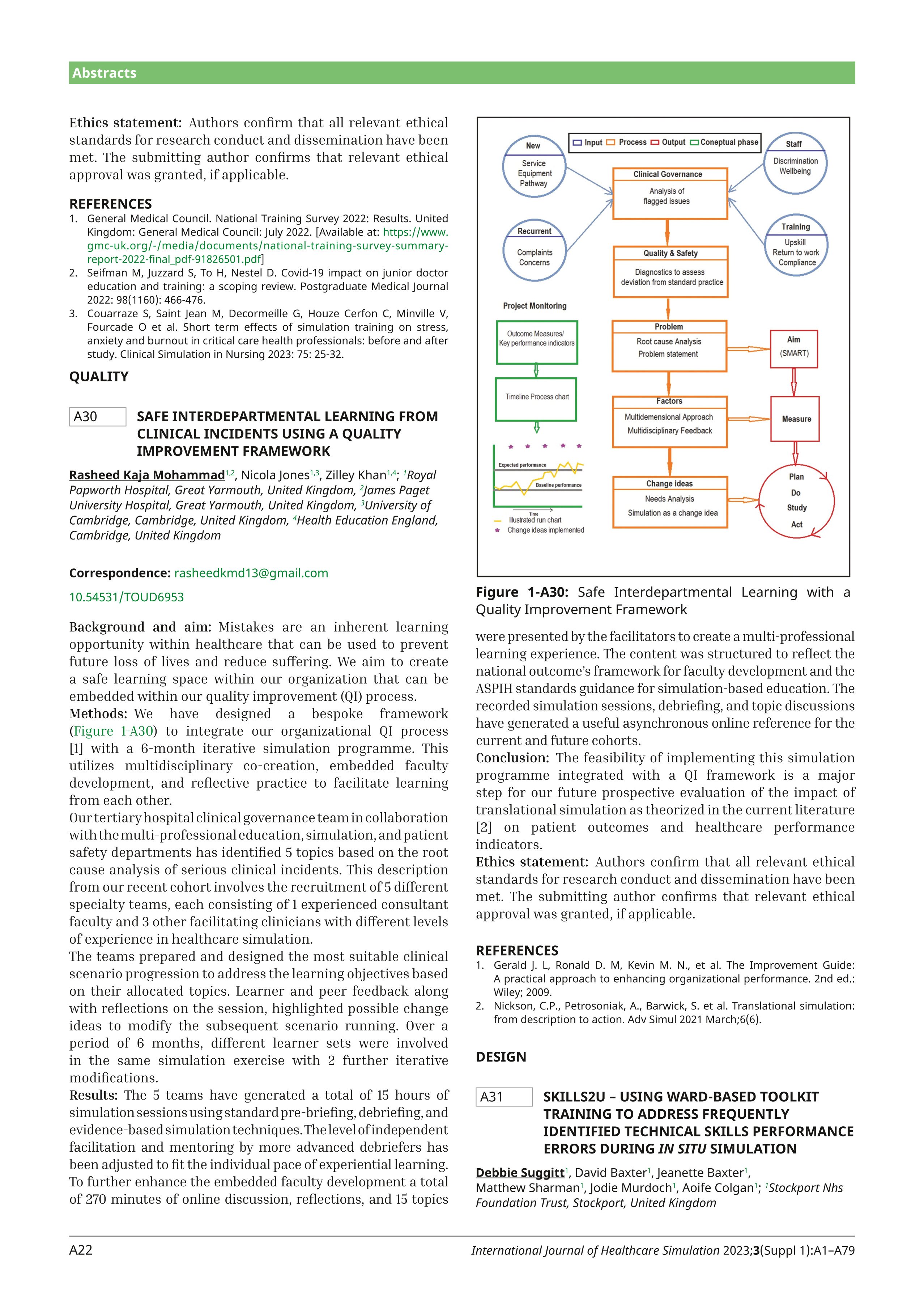
We have designed a bespoke framework (Figure 1-A30) to integrate our organizational QI process [1] with a 6-month iterative simulation programme. This utilizes multidisciplinary co-creation, embedded faculty development, and reflective practice to facilitate learning from each other.


Our tertiary hospital clinical governance team in collaboration with the multi-professional education, simulation, and patient safety departments has identified 5 topics based on the root cause analysis of serious clinical incidents. This description from our recent cohort involves the recruitment of 5 different specialty teams, each consisting of 1 experienced consultant faculty and 3 other facilitating clinicians with different levels of experience in healthcare simulation.
The teams prepared and designed the most suitable clinical scenario progression to address the learning objectives based on their allocated topics. Learner and peer feedback along with reflections on the session, highlighted possible change ideas to modify the subsequent scenario running. Over a period of 6 months, different learner sets were involved in the same simulation exercise with 2 further iterative modifications.
The 5 teams have generated a total of 15 hours of simulation sessions using standard pre-briefing, debriefing, and evidence-based simulation techniques. The level of independent facilitation and mentoring by more advanced debriefers has been adjusted to fit the individual pace of experiential learning. To further enhance the embedded faculty development a total of 270 minutes of online discussion, reflections, and 15 topics were presented by the facilitators to create a multi-professional learning experience. The content was structured to reflect the national outcome’s framework for faculty development and the ASPIH standards guidance for simulation-based education. The recorded simulation sessions, debriefing, and topic discussions have generated a useful asynchronous online reference for the current and future cohorts.
The feasibility of implementing this simulation programme integrated with a QI framework is a major step for our future prospective evaluation of the impact of translational simulation as theorized in the current literature [2] on patient outcomes and healthcare performance indicators.
Authors confirm that all relevant ethical standards for research conduct and dissemination have been met. The submitting author confirms that relevant ethical approval was granted, if applicable.
1. Gerald J. L, Ronald D. M, Kevin M. N., et al. The Improvement Guide: A practical approach to enhancing organizational performance. 2nd ed.: Wiley; 2009.
2. Nickson, C.P., Petrosoniak, A., Barwick, S. et al. Translational simulation: from description to action. Adv Simul 2021 March;6(6).
 A30Safe Interdepartmental Learning from clinical incidents using a Quality Improvement Framework
A30Safe Interdepartmental Learning from clinical incidents using a Quality Improvement Framework
 Twitter
Twitter Facebook
Facebook WhatsApp
WhatsApp LinkedIn
LinkedIn
 Tweets
Tweets