
Premature infant thermoregulation is a critical, yet challenging, component of neonatal resuscitation. Admission hypothermia is associated with multiple negative outcomes in very low birth weight (VLBW) infants. This study assessed the effect of a thermoregulation-focused simulation intervention on VLBW infant’s initial admission temperatures within a level 4 neonatal intensive care unit.
Seven multidisciplinary simulations were run in 2018 involving multiple members of the neonatal resuscitation team and led by neonatal fellows. Admission temperatures, gestational age, birth weight, maternal chorioamnionitis, antenatal steroids, caesarian section rate and need for intubation during the initial resuscitation were compared from 2019, the year following the simulation intervention, to 2017, the year preceding the simulation. Simulation participant data were collected.
Admission temperatures in VLBW infants increased from 36.0°C in 2017 to 36.5°C in 2019 following the simulation intervention (p < 0.01). There was no significant difference in birth weight, gestation age, antenatal steroids, caesarian section rate, or need for intubation in the delivery room. There was an increased occurrence of maternal chorioamnionitis in 2019 compared with 2017 (p < 0.01).
This study demonstrated that the initiation of a thermoregulation simulation intervention has the potential to improve VLBW infant admission temperatures and supports the benefits of simulation-based training.
Very low birth weight (VLBW) infants, defined as a birth weight of less than 1500 g, face considerable difficulties with maintaining normothermia due to a high surface area to body ratio and heat loss via conduction, evaporation, convection and radiation [1–4]. Maintaining neonatal normothermia is of high importance during the initial resuscitation of premature infants, and the relationship between hypothermia and premature infant mortality has been known for over 60 years [5]. For every 1°C decrease below 36.5°C, mortality increases by 14.3% [6]. In addition, admission hypothermia in VLBW infants has been associated with necrotizing enterocolitis, retinopathy of prematurity, sepsis and bronchopulmonary dysplasia [7–10].
The World Health Organization (WHO) defines euthermia within the range of 36.5–37.4°C [11]. The attainment of admission normothermia remains a challenge for VLBW infants. Strategies to mitigate admission hypothermia in newborn VLBW infants include the use of radiant warmers, use of exothermic chemical mattresses, immediate placement of infant within polyethylene bags, placing a hat on the infant’s head and increasing the room temperature to between 23 and 25°C [12,13]. Neonatal ‘Golden Hour’ admission protocols have also been developed to support the management of these infants [14–16]. While protocols and algorithms often inform participants of the required steps, they do not always address the complex technical skills or the effective communication skillset required by the resuscitation team members and leaders to manage VLBW thermoregulation.
Simulation-based education has been shown to improve teamwork behaviours, non-technical skills and leadership ability, as well as procedural skills [17,18]. The team leader is a particularly important role. Team leadership has been found to influence the quality of the technical performance of teams [19], patient outcomes, patient safety and quality of care [20]. It is also suggested that team leadership may even influence patient mortality and survival rates [21].
There are examples of the effectiveness of simulation-based training in neonatology to improve resuscitation performance and improve admission hypothermia in the community and inpatient settings [22–24]. Therefore, the aim of this study was to evaluate whether the introduction of a simulated VLBW infant thermoregulation intervention, with a particular focus on the team leader, could improve initial admission temperatures within a level 4 academic neonatal intensive care unit (NICU).
A level 4 university-affiliated neonatology unit.
Pre–post-intervention study design with retrospective review of clinical results.
Simulation teams were led by seven neonatal fellows matriculating during the year 2018. The remainder of the resuscitation team was comprised of a convenience sample of multidisciplinary clinical providers within the NICU, including paediatric residents, nurse practitioners, respiratory therapists, medical students, NICU nurses, transport nurses and family medicine residents. Participants all provided resuscitation care as part of their duties in the NICU. Determination of the specific roles of these providers was left to the team leader. All participants were Neonatal Resuscitation Program (NRP)-certified, except for the medical students. Each participant participated only once during the study period. Our training programme has seven total neonatal fellows.
The intervention consisted of a multidisciplinary simulation focused on the initial thermoregulation of a VLBW infant. Simulations were scheduled during normal work hours and were run throughout the year. Seven separate simulations were run throughout 2018. The first simulation was run in January 2018, and additional simulations were run in March, May, July and December of the same year. Each simulation and debriefing took approximately 90 minutes.
A specific simulation scenario, based on actual clinical encounters, was written to encompass the use of five crucial thermoregulatory interventions necessary to maximize temperature control in a VLBW infant (exothermic mattress, immediate use of plastic wrap, placement of infant hat, control delivery room temperature and use of a radiant warmer). The simulation scenario was written and edited by team members with training in simulation design. The objectives of the simulation were to provide the neonatal fellows and resuscitation team members with practice in the steps required to (1) prepare clinical teams for the delivery of a VLBW infant, (2) resuscitate and provide thermoregulation and (3) admit and stabilize the infant.
Following participant introductions, the simulation began with a pre-brief to orient the participants to the environment and the simulator capabilities and to review the ground rules of simulation. Specific learning objectives were not shared prior to the simulation with the participants. The team was informed that they would be notified to attend the delivery of a 26-week premature infant being delivered due to maternal pre-eclampsia. The neonatal fellows were asked to assign roles to the team members, ensure the team had the necessary equipment and prepare the team for the resuscitation. The simulation occurred in two adjacent but separate rooms within the NICU in-house simulation centre.
Upon entering the room, the team encountered a confederate who assumed the role of the delivering obstetrician. The confederate provided the team a pre-delivery briefing that included pertinent clinical information related to maternal history and the impending clinical scenario. The team was provided time to set up the warmer bed, check and prepare their equipment, and set an appropriate delivery room temperature. Of note, prior to the simulation, the thermostat in this room was turned down below 20°C. When the team was ready, the confederate would indicate that the infant was born.
Following the birth of the infant, the team began the resuscitation following NRP guidelines. The Premature AnneTM infant mannequin (Laerdal Medical) would initially be vigorous with a strong cry. Infant vigour and cry were conveyed with a verbal prompt, as the simulator does not have the ability to physically express these signs. When monitoring leads were initially placed on the infant, vital signs displayed were heart rate (HR) of 150, respiratory rate (RR) of 60 and oxygen saturations of 75% at ~1 minute of life. Over time the infant’s RR and HR decreased, requiring the team to select the most appropriate respiratory intervention, ranging from delivery of positive pressure ventilation to intubation. Vital signs were adjusted via a Laerdal sim pad and displayed on a Laerdal monitor in response to the team’s efforts to stabilize the infant. Following intubation and stabilization of the infant’s HR and saturation, the team would transport the infant on the warmer bed from the simulated labour and delivery room back to NICU simulation centre.
Infants were admitted to a simulated NICU room within the simulation centre. The infant was transferred from the transport warmer to a Giraffe warmer bed. Infant weight and temperature needed to be immediately obtained. The admission temperature was assigned to the mannequin based on the number of temperature stabilization steps that were included within the initial resuscitation. Goal admission temperature was achieved if all key thermoregulation steps, including monitoring and adjusting the room temperature, were performed. If all five components were completed, then the assigned infant’s simulated admission temperature would be above 36.5°C; if any of the steps were omitted, then the temperature would be 36.0°C.
The team was debriefed by simulation team personnel with specific training in debriefing. The debrief occurred immediately following the scenario and followed the CAPE Technical Performance Debriefing Method developed and taught at the Center for Advanced Pediatric and Perinatal Education (CAPE) [25]. Specific attention was paid to the steps required to provide thermoregulation in a VLBW infant. This included discussion of radiant warmers, exothermic mattresses and polyethylene bags; placing a hat on the infant’s head; and increasing the room temperature to between 23 and 25°C. Fellows were informed that the room temperature had been turned down prior to the simulation. Debrief also explored critical thinking, leadership, technical skills, protocol recognition and team performance (Figure 1). Each individual simulation was debriefed by the same two, trained individuals. Debriefing time ranged from 30 to 45 minutes. No specific data were collected during the debriefing period.

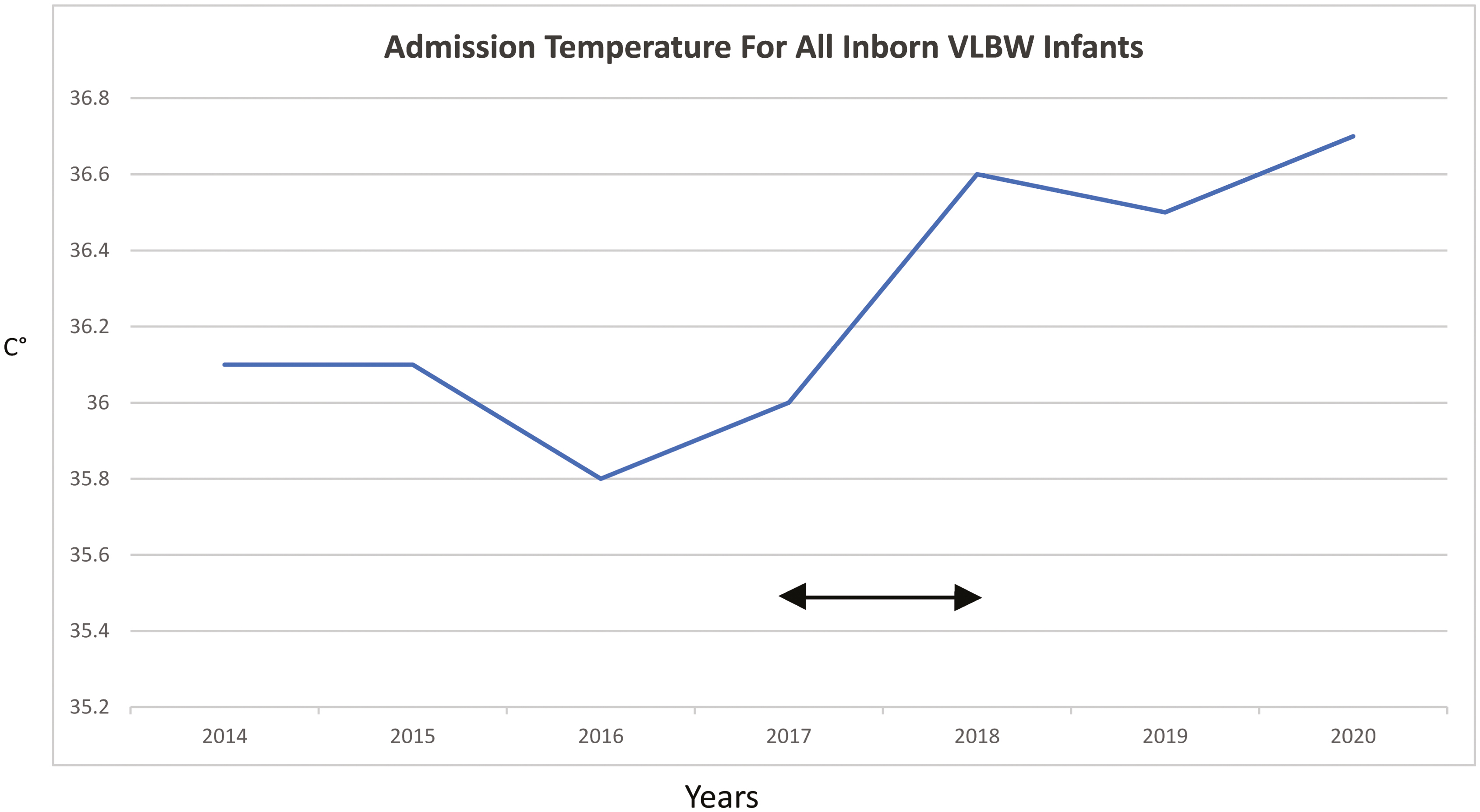
Initial admission temperatures of VLBW infants across time.
The performance of all team members was assessed according to three domains: (1) critical thinking and situational awareness, (2) leadership and communication and (3) technical skills and protocol recognition (Table 1). Particular attention was focused on the fellow’s level of performance in the role of team leader. An evaluator assessed whether the team had performed the critical steps of thermoregulation. Following the simulation, fellows were also asked to rate the effectiveness of the simulation and whether it had an impact on their clinical behaviour in a post-simulation survey distributed after their participation. Fellow simulation reaction data were collected in the form of a survey given to the fellows following the simulation.

| Critical Thinking and Situational Awareness: |
| 1. Radiant warmer 2. Exothermic warmer mattress 3. Room temperate 4. Polyethylene wrap immediately applied 5. Neonatal hat 6. Decision made to intubate 7. Generate admission plan |
| Leadership and Communication |
| 1. Discussion of team roles 2. Clear, direct and closed-loop communication 3. Showing infant to mother prior to leaving room |
| Technical Skills and Protocol Recognition |
| 1. Set up and check equipment prior to delivery 2. Asking for delayed cord clamping 3. Intubation attempts 4. Obtain a weight upon admission |
The gestational age, birth weight and admission temperature of inborn neonates weighing less than 1500 g born in the hospital during the year prior to the intervention (1 January 2017 until 31 December 2017) and in the year after the intervention (1 January 2019 until 31 December 2019) were compiled from EPIC and the Vermont Oxford Network (VON). All VON data were site-specific, and data were collected in accordance with the data definitions governed by VON. VON is a non-profit collaboration comprised of NICUs across the world. Additional measures obtained from the database included antenatal steroid use, maternal chorioamnionitis, birth by caesarian section and intubation within the delivery room. Additionally, mean inborn admission temperatures were obtained from the Vermont Oxford Database across a 7-year period (Figure 1).
All data were analyzed on GraphPad Prism 8. The primary outcome measure was the infants’ admission temperature. Gestational age, initial temperature and birth weight were compared pre- and post-intervention using Mann–Whitney testing for non-parametric continuous variables. Chi-squared testing was employed to compare the percent of infants born with an initial admit temperature less than 36.0°C, maternal chorioamnionitis, caesarian sections, antenatal steroid use and intubation in the delivery room. The effect size was determined using Cohen’s delta. No major changes in the NICU’s thermoregulation policy occurred across the study time period, and no new thermoregulation equipment was employed.
In total, seven VLBW thermoregulation and admission simulations were run from January through December 2018, and teams were comprised of 7 neonatal fellows and 38 clinical team members made up of paediatric residents, nurse practitioners, respiratory therapists, medical students, NICU nurses, transport nurses and family medicine residents. Each simulation involved only a single fellow. Additional team members represented a wide range of clinical experience, ranging from many years to new hires.
All participating teams missed one or more steps of thermoregulation, resulting in all infants receiving an assigned initial temperature of less than 36.5°C. All seven participating fellows rated the simulation highly (score = 5) with respect to its ability to provoke a change in clinical behaviour and the effective learning it provided. They rated the experience a positive one (Table 2).
| Fellow Checklist Performance | Average Successful Thermoregulation Steps Average Admit Temperature |
3/5 36.0 |
| Fellow Evaluation 5-point Likert Scale |
Simulation Realism Simulation was a Positive Experience Simulation Provided Effective Learning Simulation Produced Changes in Clinical Behaviour Overall Evaluation of Simulation |
4.8/5 5/5 5/5 5/5 5/5 |
N = 7 neonatal fellows. No runs of the simulation demonstrated all five thermoregulation steps. Fellow evaluation of the simulation was supportive.
There was no difference in infant size, gestation age, birth weight, receipt of antenatal steroids or requirement of intubation within the delivery room between the two comparison groups.
There were 129 VLBW infants born in the year prior to the intervention, with a mean admission temperature of 36.0°C, and 122 born in the year after the intervention, with a mean admission temperature of 36.5°C (Table 3). The difference in temperatures was found to be statistically significant. The effect size of the difference was 0.64 using Cohen’s delta, which falls in the medium effect size range. The percent of admissions with infant temperature under 36.0°C decreased from 47.6% in the year prior to the intervention to 19.6% in the year after the intervention (Table 3). The percent of infants whose mothers were diagnosed with chorioamnionitis was significantly higher in 2019 than in 2017. Mean temperatures for infants born less than 700 g were not found to be significantly different between the two time points and were below the goal admission range.
| Admission temperature °C, mean (SD) | Admission temperature with maternal chorioamnionitis °C, mean (SD) | Admission temperature without maternal chorioamnionitis °C, mean (SD) | p-value | |
|---|---|---|---|---|
| Year prior to the intervention 2017 | 36.0 (0.75) | 36.4 (0.74) | 36.0 (0.74) | 0.06 |
| Year following completion of the intervention 2019 | 36.5 (0.81) | 36.4 (0.88) | 36.5 (0.79) | 0.53 |
Infants born in the year 2017 (pre-simulation intervention) compared with the year 2019 (post-simulation intervention). SD = standard deviation. Significance determined if p < 0.05.
In light of the significant increase seen in infants born to mothers with chorioamnionitis between the 2 years, a sensitivity analysis was performed to assess its impact on admission temperatures. The presence of maternal chorioamnionitis had no statistical significance on mean admission temperatures, and no difference was seen either year between infants born with maternal chorioamnionitis and those born without chorioamnionitis (Table 4).
| Year prior to the intervention 2017 | Year following completion of the intervention 2019 | p-value | |
|---|---|---|---|
| Total infants | 129 | 121 | |
| Birth weight, g, mean (SD) | 1022 (315) | 1025 (327) | 0.90 |
| Gestational age, weeks, mean (SD) | 28 (3.1) | 27.28 (3.0) | 0.20 |
| Admission temperature, °C, mean (SD) | 36.0 (0.75) | 36.5 (0.81) | 0.01 |
| Admission temperature, °C (birth weight <700 g), mean (SD) | 35.62 (0.87) N = 23 |
35.87 (1.2) N = 27 |
0.17 |
| Infants with initial admission temperature below 36.0°C, n (%) | 52 (40.3) | 24 (19.7) | 0.01 |
| Antenatal steroids, n (%) | 131 (98.5) | 119 (98.2) | 0.96 |
| Caesarean section delivery, n (%) | 133 (75.9) | 87 (71.3) | 0.74 |
| Maternal chorioamnionitis, n (%) | 14 (10.5) | 36 (29.8) | 0.01 |
| Male sex, n (%) | 65 (48.9) | 69 (56.6) | 0.49 |
| Intubated within the delivery room, n (%) | 66 (49.6) | 72 (59.0) | 0.41 |
Infants born with maternal chorioamnionitis and without chorioamnionitis in 2017 and 2019 did not demonstrate a significant difference in initial admission temperatures. SD = standard deviation. Bold values indicate statistical significance with p values less than 0.05.
The introduction of a simulation focused on inborn VLBW infant thermoregulation resulted in improved initial admission temperatures in a level 4 academic hospital. Maintaining neonatal normothermia is of high importance during the initial resuscitation of premature infants and requires the coordination of both technical and non-technical skills by the members of the resuscitation team. At our centre, the NICU is adjacent to the labour and delivery department. Our unit protocol is to have all VLBW infants resuscitated, intubated, stabilized and admitted within 15 minutes of delivery to the NICU. There is no use of a temperature probe during our resuscitation, and there is no pre-warming of infants prior to admission. The first temperature obtained is at the time of actual NICU admission, and infants found to be below the goal temperature are warmed accordingly. The use of temperature probes and pre-warming with servo control mode prior to admission to the NICU has been used in other studies to successfully improve temperatures prior to admission [24,26]. It is important to view the improvement in our admission temperatures through this lens. Improvements in admission temperatures, therefore, are likely to be reflective of improved thermoregulation during the resuscitation.
While admission temperatures are the result of a complex multifactorial process, no other changes in NICU policy occurred during the study period to address admission hypothermia. Although there were new faculty hires and new fellows that spanned the two time periods, there were no major shifts in admission algorithms, measurable team behaviour, educational curriculum focused on admission temperatures or thermoregulation policies. There were no quality improvement initiatives or any implementation of strategic plans to reduce admission hypothermia. Infants were of similar size and gestational age at birth between the two epochs; therefore, any improvement in temperature cannot be attributed to discordance in patient size or maturity between epochs. Clinically, the magnitude of improvement in admission temperatures by 0.5°C resulting in achieving a mean goal of 36.5°C is striking. The WHO defines admissions temperatures falling in the range of 36.0–36.4°C as cold stress or mild hypothermia [27]; therefore, the improvement to a goal temperature above this threshold is likely to be clinically relevant. Data from the Canadian Neonatal Network demonstrated that admission temperatures below 36.5°C were associated with infection, bronchopulmonary dysplasia, retinopathy of prematurity and neurologic injury [7]. In addition, preterm infants born at temperatures less than 36.5°C have an increased risk of in-hospital mortality [28]. Raising our admission temperatures above this key threshold may have significant ramification on VLBW outcomes.
The mean admission temperatures of 36.54°C in 2018, the year the intervention occurred, and of 36.5°C in 2019 represent overall improvements when compared with a previous retrospective study performed at our institution of 504 VLBW infants for over a 5-year period. This study found the mean admission temperature of VLBW infants to be 35.8°C, and only 19% were admitted with normothermia [29]. Additionally, this improvement from historic temperatures has been maintained (Figure 1), and the simulation is now a part of our educational curriculum and a component of our approach to providing medical care for VLBW infants [30]. This study highlights the potential clinical impact of a simulation-based intervention and the importance of scientific interrogation. The broader impact of simulation on clinical scenarios is an important, yet understudied, programmatic goal.
Infants born in the 2019-time epoch were more likely to have mothers diagnosed with chorioamnionitis. Chorioamnionitis is associated with temperature dysregulation in premature infants and has a complex relationship with admission temperatures. Infants born at greater than 35 weeks’ gestation to mothers diagnosed with chorioamnionitis have demonstrated admission hyperthermia [31,32]. This relationship becomes less clear in premature and VLBW infants. Multiple studies looking at preterm infants have demonstrated that chorioamnionitis may promote normothermia [33,34], may promote hyperthermia or may have no relationship with admission hypothermia [2]. It is important to view the results of the simulation intervention in this context. To remove the potential confounding effect of chorioamnionitis, we performed a sensitivity analysis to assess whether it had an impact on our population on admission temperatures. No difference was seen in overall mean admission temperatures, admission temperatures of infants born with maternal chorioamnionitis and infant born without the involvement of chorioamnionitis in either of the two epochs. Despite the complex relationship between chorioamnionitis and temperature dysregulation, this finding suggests that an increase in maternal infection in 2019 did not influence the improvement in admission temperatures in a meaningful way. This lends additional support that the simulation intervention contributed to the improvement in admission temperatures.
Admission temperatures were likely improved through several mechanisms. The experiential learning and focused feedback received by the neonatal fellows and team members performing the simulation potentially improved their clinical behaviour when admitting real VLBW infants. Neonatal fellows attend all VLBW deliveries at our centre and fill the primary team leader role in the majority of VLBW resuscitations, so influencing their behavior affects nearly every VLBW admitted to the NICU. Shortcomings in leadership behaviour have been associated with perinatal morbidity; therefore, emphasis was placed on fellow leadership skills [35]. While leadership training is a crucial aspect of neonatal graduate medical education, all individuals who participated received focused debriefing and performance evaluation. While the fellows train for a 3-year period before starting their careers, the additional team members involved in the simulation often provide more continuity within the NICU. Therefore, lessons learned by the multidisciplinary team through the simulation and debrief likely influenced the clinical impact of improved admission temperatures. Team training in neonatology leads to improved resuscitation [36–38]. It has been demonstrated that having an individual team member who has participated in a previous simulation educational experience that was focused on the prevention of admission hypothermia resulted in improvement in a new team’s performance [23]. Thirty-eight additional team members who were able to participate in the simulation, therefore, had the opportunity to bring their training experience back into the clinical environment. The team training aspect of the simulation represents an additional mechanism that likely contributed to the increase in admission temperatures. Raising attention and focus on the use of thermoregulation equipment and immediate placement of plastic wrap likely provided more clinical benefits as well. Additional research is needed to determine the specific components of the simulation that resulted in the notable increase in admission temperatures. At our institution, neonatal fellows attend all high-risk deliveries and are most frequently delivery team leaders. Training resuscitation teams in the skills needed for VLBW thermoregulation appears to be a strong method for improving unit admission temperatures. In our study, an overall improvement in admission temperatures was not seen in infants born weighing under 700 g. This represents an area that needs increased attention, as these infants are at the greatest risk.
The relative infrequency with which resuscitation team members are given the opportunity to manage VLBW infants, estimated at 1.5% of the total birth per year in the USA [39], creates substantial challenges in both acquiring and maintaining the skills required to manage these infants. Therefore, as is the case for other neonatal resuscitation scenarios, the use of simulation has become increasingly commonplace as an approach to provide training in these high-risk and low-frequency events [40].
It is not common to evaluate the impact of simulation-based interventions in the clinical environment [41]. The fact that this has been carried out is a strength of this study. Typically, it has been found that assessments of the effect of team training on clinical processes or patient outcomes sizes have tended to fall in the medium to large range [42]. The effect size within this study of 0.64 was found to be of medium value, with 73.9% of the cohort of infants born in 2019 following the introduction of the simulation curriculum mean admit temperatures being above the control group infant’s mean temperature. There has been some suggestion that when assessments of the effectiveness of team training are made in the clinical environment they may lack explicit plausibility for causation [43], as the outcomes are too removed from the intervention for any meaningful impact of one on the other to be evident [41]. We posit that this is not the case in our study, which has a meaningful clinical outcome variable (i.e. admission temperature). We recommend that other researchers give careful consideration to the clinical measures of effectiveness they use to ensure that they have explicit plausibility for causation.
Another strength of this study is the use of clinical parameters to evaluate the effect of a simulation-based intervention. It is often difficult to link simulation with clinical change, despite this being an assumed goal of simulation [44]. This study represents an operationalized example of what many refer to as translational simulation, with a simulation-based intervention [45,46]. The clinical improvement in admission temperatures also supports the fellows’ self-evaluations stating that there was effective learning occurring and that the simulation promoted clinical change, as a significant clinical change in admission temperatures was in fact ultimately seen.
Several studies have looked at the effect of the implementation of a neonatal admission and thermoregulation protocol, often involving simulation and team training, on the premature infant admission temperatures [47,48]. Our study approaches thermoregulation from a different perspective. We have had a golden hour protocol in place since 2012; therefore, simulation was the single intervention initiated to improve admission temperatures. The simulation was designed by neonatologists with specific simulation training, providing strong content validity within a very specific clinical context. The simulation is reproducible, and this study is replicable. The sustained success of the simulation across several years represents an additional strength of the study. While self-reported outcomes frequently contain bias, the fellows’ rating of the simulation is consistent with the improvement in outcome measures. An assessment metric less associated with bias and provided to all team members would have strengthened this aspect of the study and is being planned for future work.
A potential limitation of the study is the lack of long-term outcome clinical data. Assessing outcomes data from the neonates involved would make for exciting future work but was beyond the scope of this project. Additionally, the study assessed seven runs of the simulation over the course of a year at a single centre, and the question can be asked whether this was sufficient volume to create the results seen within the study. It is important to note, though, that these seven runs involved the neonatal team members most likely to attend and lead the resuscitation of VLBW infants. Focusing the simulation intervention on neonatal fellows and the resuscitation nurses who attend the high-risk deliveries increases the yield of the intervention considerably. However, we were not able to train every resuscitation nurse with this intervention. Furthermore, we were unable to standardize the team members. Therefore, some teams involved more experienced fellows and nurses, while others did not. While this lack of standardization had effect on the simulation (teams comprised of more experienced clinicians may have had improved simulation performance), in a real-world setting, it is important that neonatal resuscitation teams function at a high level regardless of their composition. Though simulation has become a standardized part of the fellows’ educational curriculum, future work could still be directed as further assessment from a more formalized quality improvement approach. Additional focus on improving admission temperatures for infants born with birth weights less than 700 g, a group that did not have a perceivable increase in admission temperature, is a future direction of this work. This lack of improvement could be a function of small numbers, reflective of a more tenuous physiology or reflective of systemic issues that need to be further addressed. An additional limitation is that there is no way to account for the additional learning that may occur throughout a NICU at any given point in time surrounding any given topic, specifically in this context of thermoregulation. Future studies would also benefit from a prospective assessment, as the retrospective nature of this work is an additional limitation, though one driven by feasibility.
Although VLBW birth is not a common event, it is important to ensure that neonatal resuscitation teams have the skills required to achieve neonatal normothermia in this population. This study demonstrated that the introduction of a thermoregulation simulation within a NICU has the potential to improve VLBW infant admission temperatures, and it provides support for the need, and benefits, of simulation-based training for these high-risk/low-frequency events.
All authors participated in the design, editing and writing of the study. All authors approved the final manuscript. TGE, GR, ES and POC designed the study. TGE and TTC extracted the data, interpreted the results and wrote the manuscript. TGE extracted the data and edited the manuscript. MS and ES assisted with content and revision. TGE and TTC conducted the statistical analysis of the data, interpreted the results and created the figures.
This work was supported by the University of Iowa (University of Iowa Graduate Medical Education Innovation Grant to TGE).
None.
Ethical approval for the study was obtained from the University of Iowa Institutional Review Board (201903826).
The authors declare that they have no conflicts of interest.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
 The introduction of a simulated thermoregulation intervention to improve very low birth weight infant initial admission temperatures in a neonatal intensive care unit
The introduction of a simulated thermoregulation intervention to improve very low birth weight infant initial admission temperatures in a neonatal intensive care unit
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
 Tweets
Tweets