
Paediatric vascular access can be notoriously difficult due to small vessels and patient cooperation. Studies have shown ultrasound (US) guided technique to be a more successful method in experienced hands, especially in children with difficult access [1]. US-guided vascular access is well established within adult medicine; however, at present there is no standardized practice in paediatrics with many clinicians not gaining any US experience, unless undertaking acute sub- specialist placements [2]. In some cases, children are transferred to tertiary centres where there is more US expertise [2]. To enable the best patient care within their local setting, US skills should be routinely taught to all paediatricians.
To date, there have been no studies exploring the experience and significance of US-guided vascular access training amongst district general hospital (DGH)-based UK paediatricians. We aimed to evaluate this within our DGH.
Small-group US vascular access simulation sessions were led by our accredited and experienced paediatric advanced nurse practitioner (ANP). Participants learned to map veins and practiced US cannulation technique on the gelatinous ‘phantom’ model. A questionnaire asked attendees to evaluate confidence levels before and after sessions, and open-space for qualitative comments.
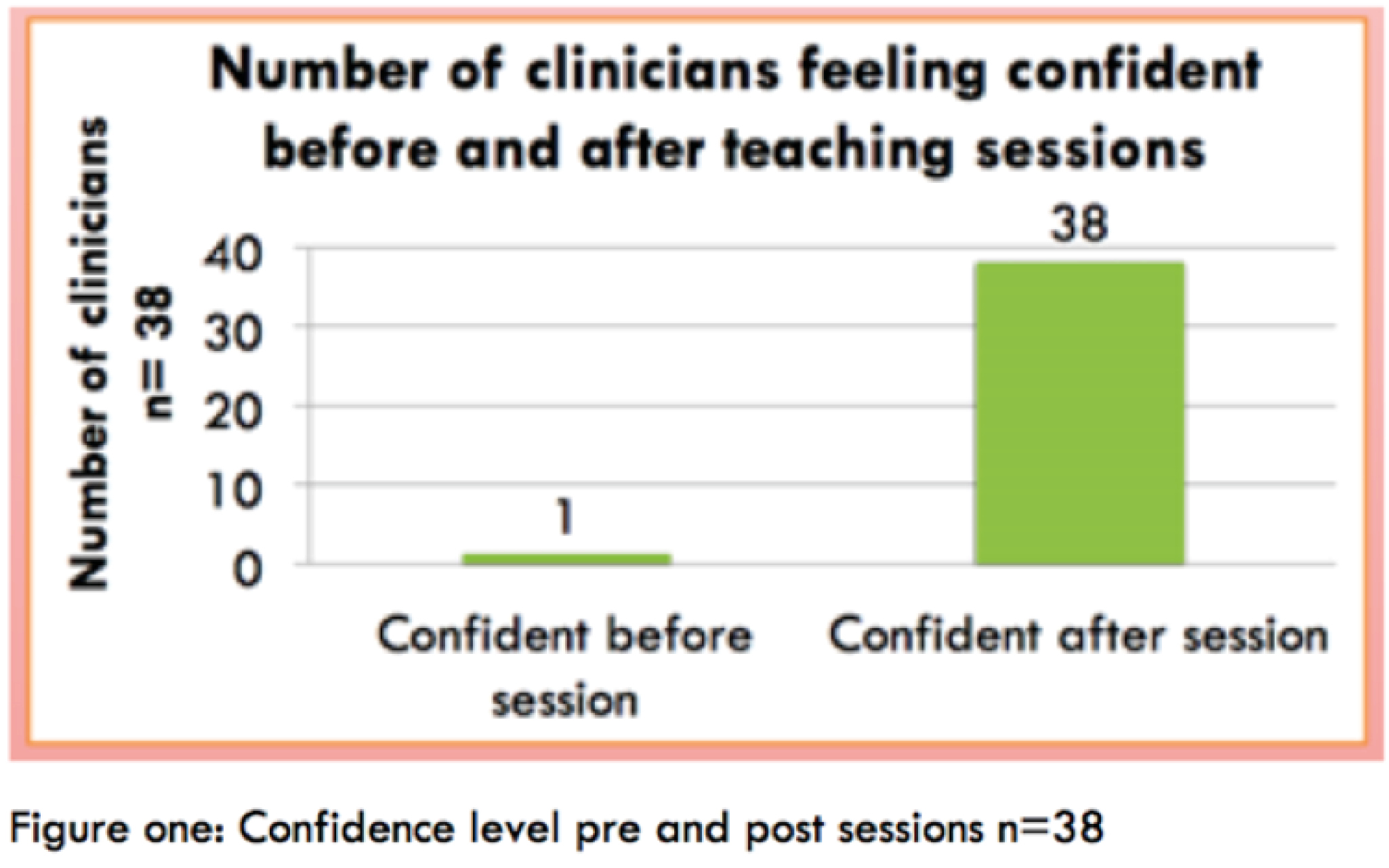
Thirty-eight paediatricians attended sessions; of whom, 75% had never conducted US vascular access and 96% did not feel confident. Following sessions, 100% of participants felt significantly more confident and would attempt this on real patients (Figure 1). Qualitative comments showed that they valued sessions: ‘good opportunity to practice vein mapping and cannulation on gel model’. All participants felt that this should be taught routinely within paediatric training. Five participants used this new skill in real patients, following the sessions.

This study demonstrates the effectiveness and usefulness of delivering US-guided vascular access training to DGH paediatricians. It enabled improved self-reported confidence, which translated into improved patient care in real-life scenarios. Following its success, we intend on running this as an ongoing session. For clinicians wanting to utilize their skill on real patients, this will be supervised by our ANP. We recommend that all UK paediatricians train in US vascular access to enable optimal care for paediatric patients in all hospital settings. However, further research in a larger cohort of participants is required. We also recognize the variability in available expertise and equipment in all units to undertake the training. The importance and role of US-guided paediatric vascular access are still lacking in recognition and demands wider acceptance.
1.
2.
 16 Exploring the Benefits of Teaching Ultrasound-Guided Vascular Access to Paediatricians
16 Exploring the Benefits of Teaching Ultrasound-Guided Vascular Access to Paediatricians
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
 Tweets
Tweets