
Resuscitation teams in emergency departments are ad hoc teams who perform life-saving treatment with little or no preparation time. Logan Hospital Emergency Department (ED) is one of the busiest in Australia and has a high staff turnover. Simulation team training impacts on and can improve team relations [1] and is effective at improving learner’s knowledge, attitudes and behaviours [2]. Increased team familiarity has been shown to improve team performance [3,4].
The Resus Drills project aimed to increase team familiarity and establish regular, supported practice of local protocols and important resuscitation topics. These aims were evaluated by surveys exploring participants’ perceptions of the usefulness of the drills and measuring if confidence had increased.
The Logan ED streams patients to different areas and teams. The resuscitation team gathered in one of the resuscitation bays at the beginning of each Monday to Friday day shift (when patient care allowed) for team member introductions (name and role) followed by a short simulation education session. These Resus Drills took approximately 20 minutes and were facilitated by a nurse educator and emergency consultant or simulation registrar over a three-month trial period, from 30/02/2021 to 30/06/2021. This project was exempt from full ethical review.
This project was developed in two phases: consultation, and concurrent implementation and evaluation. Consultation consisted of pre-project surveys sent to all 256 nursing and medical staff who work in the resuscitation area, yielding 54 responses (response rate of 21%). In total, 53 (98%) respondents believed that brief simulations would increase their confidence in managing clinical scenarios. Only 17 (31.5%) respondents always knew the names and roles of team members, 22 (40.7%) usually knew and 13 (24.1%) sometimes knew.
Respondents were asked to dichotomously rate confidence in managing 12 resuscitation scenarios. Staff were least confident with transcutaneous pacing (15, 27.8%), COVID-19 intubation (14, 25.9%), resuscitaire operation (12, 22.2%) and massive haemorrhage protocol (11, 20.4%); 11 scenarios were developed based on these topics and data.
A descriptive mixed-methods approach was adopted with concurrent collection of quantitative and qualitative data via self-administered anonymous surveys hosted on Microsoft FormsTM . Surveys were collected during the consultation phase and also during the evaluation phase. Surveys utilized Likert scales to quantify the perceived benefit and utility of the simulation, and free-text responses collected qualitative data. Quantitative findings were analyzed using descriptive statistics, and qualitative responses were thematically analyzed according to the approach described by Bree and Gallagher [5]. All authors independently reviewed the qualitative data, developing a code book of themes arising de novo from the data. All authors then independently coded the entire dataset before collaboratively reaching an agreement on final themes.
Post-scenario surveys were distributed via QR codes and completed either immediately or during the shift by participants on their personal devices. Post-project surveys were distributed via staff emails.
An estimated 2–3 Resus Drills were conducted each week during the project. On other weekdays, patient care did not allow the team to gather for a Resus Drill.
In total, 121 post-scenario survey responses were received, of which 108 (89.3%) reported that the Resus Drill was extremely useful, and 12 (9.9%) reported it as a bit useful.
Only 15 post-project responses were received; 13 (86.7%) respondents reported that they participated in 1–5 Resus Drills. One (0.1%) respondent reported participating in more than five simulations. 12 (75%) reported the scenarios as either useful or extremely useful. All respondents reported their confidence had increased in at least one scenario topic. Three respondents described instances in which they used what they had learned from the Resus Drills to perform clinical work.
Qualitative thematic analysis identified four themes describing how team members found the drills useful (Figure 1; Table 1). The theme of ‘simulation factors’ discussed the realism of the simulations and described a supportive environment with effective facilitation, while noting both limitations of in situ simulation and the challenge of balancing simulation participation with patient needs. Respondents discussed the benefit of context, i.e. scenarios designed to meet their learning needs.

| Theme | Example quotes |
|---|---|
| Simulation factors | ‘Background noise from the mannequin was realistic and assisted with immersion and managing communication in a more noisy background environment’; ‘ Supportive environment for learning’; ‘Able to practice skills in a calm and non-threatening environment’; ‘Hard in early mornings in resus to do a sim … most patients need things done, rooms need to be checked... Protection of sim time [needed]’ |
| The resuscitation team | ‘Getting to know the team at the start of the day and how we can improve...’; ‘Learning team names and roles’; ‘Supporting junior staff”’; ‘Good idea for people to introduce themselves at the start of the shift so people know roles’; ‘Everyone was clearly introduced with roles at the beginning with effective communication throughout’ |
| Reflection | ‘Great to … identify my learning deficits’; ‘Made me aware of areas I need to improve’; ‘Allowed me to explore areas of weakness’; ‘Good reflection on practice’ |
| Upskilling/learning – clinical knowledge | ‘Increases familiarity with local protocols’; ‘Reinforced knowledge’ ‘Great to consolidate my knowledge for [advanced life support] and hyperkalaemia’; ‘Good drug and protocol refresher’ |
| Upskilling/learning – procedural skills | ‘Good to know procedure for [COVID-19] intubation’; ‘Good to refresh skills that I hadn’t completed in a while’; ‘Use and location of splints and binders’ |
| Upskilling/learning – opportunity to practice | ‘Recap on cases which we don’t see very often’; ‘The sim we did I have never experienced on the floor’; ‘Good to run through a COVID [intubation] sim as don’t get a lot of experience to it’ |

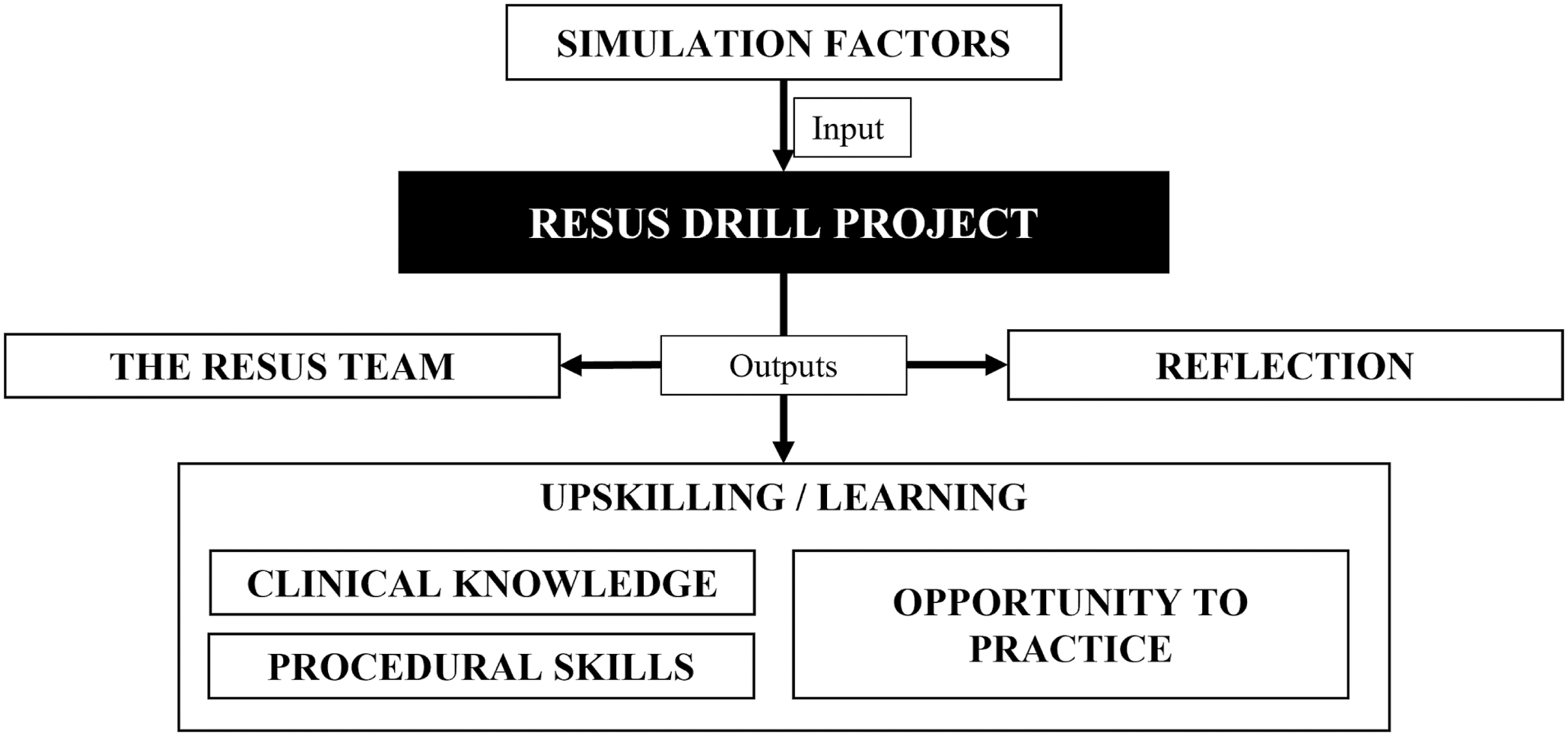
Mapping of derived themes
The remaining three themes described outputs or outcome following participation in the simulations: (1) the resuscitation team, (2) reflection and (3) upskilling/learning. Respondents described increased team and role familiarity as well as improved communication and team function. Participants reported that these brief and frequent scenarios enhanced self-awareness and encouraged further learning, in turn increasing individual confidence. Finally, the ‘upskilling/learning’ contained three prominent sub-themes: (1) clinical knowledge, (2) procedural skills and (3) opportunity to practice. These sub-themes described specific areas felt to be enhanced by participation in the drills.
The Resus Drills continued after the trial period, but feasibility decreased with COVID-19-related staff shortages and increased clinical demand. However, the benefits of this project make its continuation a key priority within the department. It is hoped that this model could be used to enhance team familiarity and function in other clinical settings. Future research with rigorous pre- and post-scenario response matching and measurement of key patient-related and team performance indicators would further support the success of similar interventions in enhancing team performance.
Sonia Twigg conceived the project idea, contributed to the ethics application and creation of surveys and scenarios, acted as a facilitator for the drills and made substantial contributions to analyzing the data and writing the manuscript. She also supervised the project. Ravi Krishna Rao wrote the ethics application, surveys and some of the scenarios; acted as a facilitator; and made substantial contributions to analyzing the data and writing the manuscript. Zachary Horn made substantial contributions to data analysis and writing the manuscript. Kirri de Kruijf contributed to the ethics application and creation of surveys and scenarios, acted as a facilitator for the drills, made substantial contributions to analyzing the data and contributed to editing the manuscript.
Thank you to the Logan Hospital Emergency Department, education team and incredible resuscitation staff for participating in and supporting this project.
None.
None.
None declared.
The authors declare no conflict of interest.
1.
2.
3.
4.
5.
ED Resus Drills – Pre-project survey
1. Do you feel confident in managing or using appropriate guidelines and protocols for the following clinical conditions. Tick all that apply
2. Do you think that a 20-minute resus sim practice during your shift will help to improve your confidence in managing these conditions?
3. Do you think that a 20-minute resus sim practice during your shift will interfere with the clinical work in resus?
4. In a resus situation, how often do you know the names of your team members and their role allocation?
5. How do you think regular sim-based resus team practice might affect team morale?
ED Resus Drills – After session survey
1. How useful was this drill?
2. How was it useful?
3. Any other feedback/comments?
4. Which scenario did you do today?
ED Resus Drills – Post-project survey
1. How many resus Drills have you participated in during the last 3 months?
2. Do you feel the Resus drills have increased your confidence in managing or using appropriate guidelines and protocols for the following clinical conditions. Tick which ones apply
3. Were the Resus Drills useful?
4. How were they useful?
5. Did the Resus Drills interfere with your clinical work?
6. How have the Resus Drills impacted on team morale?
 Daily team introductions and simulation education to improve team performance
Daily team introductions and simulation education to improve team performance
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
 Tweets
Tweets