
What? Fiberoptic intubation (FOI) is a technique used to establish airway access in patients with anticipated and unanticipated difficult airways. Fiberoptic bronchoscopes are currently used to facilitate endotracheal intubation via either the nasal or oral route, in the positioning of endotracheal and endobronchial tubes and bronchial blocking devices, and in airway examination or evaluation. FOI is used in the management of awake spontaneously breathing patients with an anticipated difficult airway [1,2]. Anaesthetic trainees require development and maintenance of flexible bronchoscopy skills for tracheal intubation. For junior trainees or those who have not had exposure to this procedure, a virtual reality simulator, the ORSIM® bronchoscopy simulator (Airway Simulation Limited, Auckland, New Zealand), has been developed. The ORSIM® simulator is designed to incorporate a virtual patient with a difficult airway. A replica bronchoscope is advanced through a black box desktop sensor, which is connected to a laptop computer and allows visualization of video bronchoscopy. The laptop software program includes upper and lower virtual airways of varying complexity. Virtual oral, nasal and conduit entry points can be selected; the program provides recording, feedback, measurement and relevant clinical data.
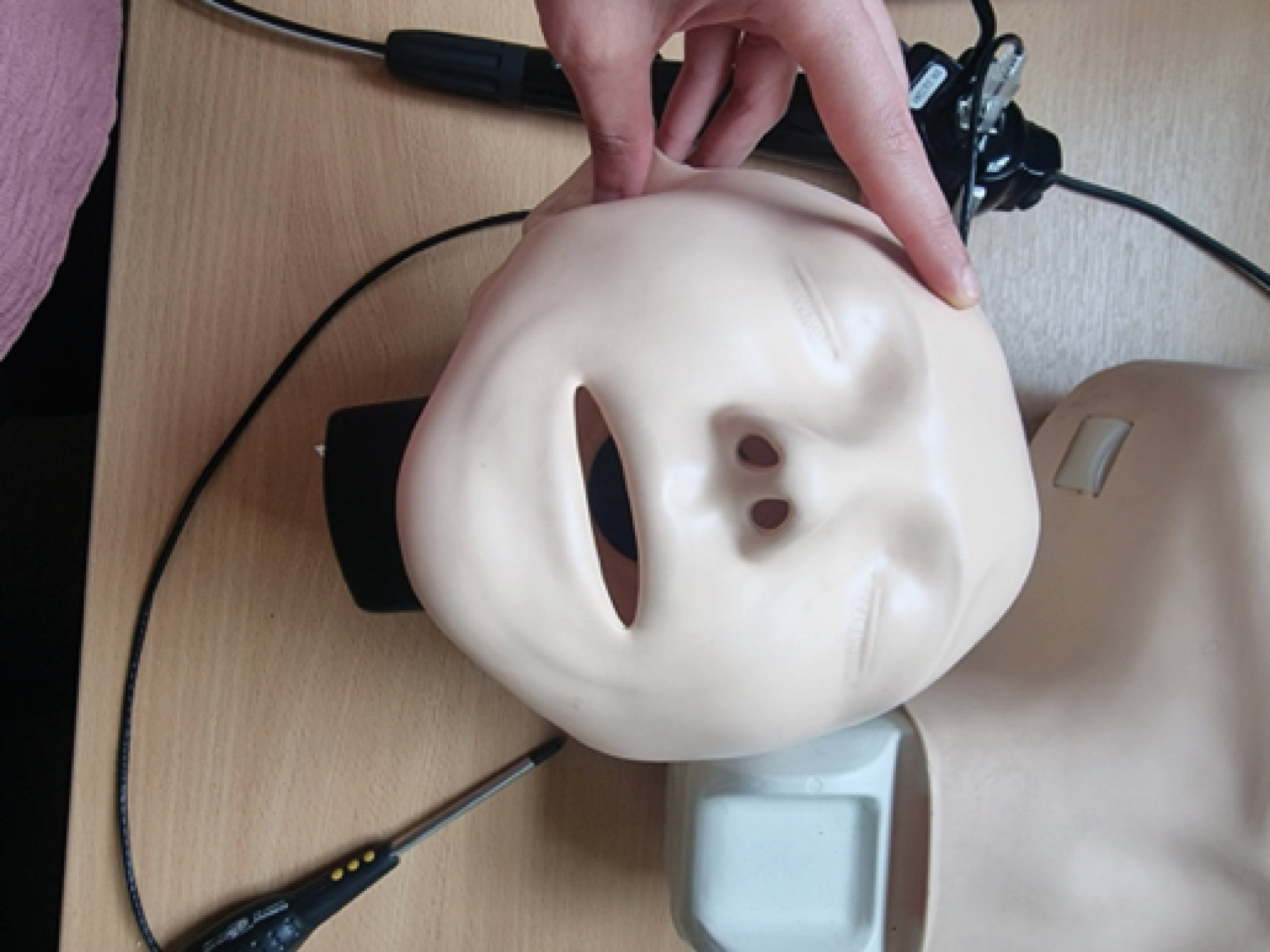
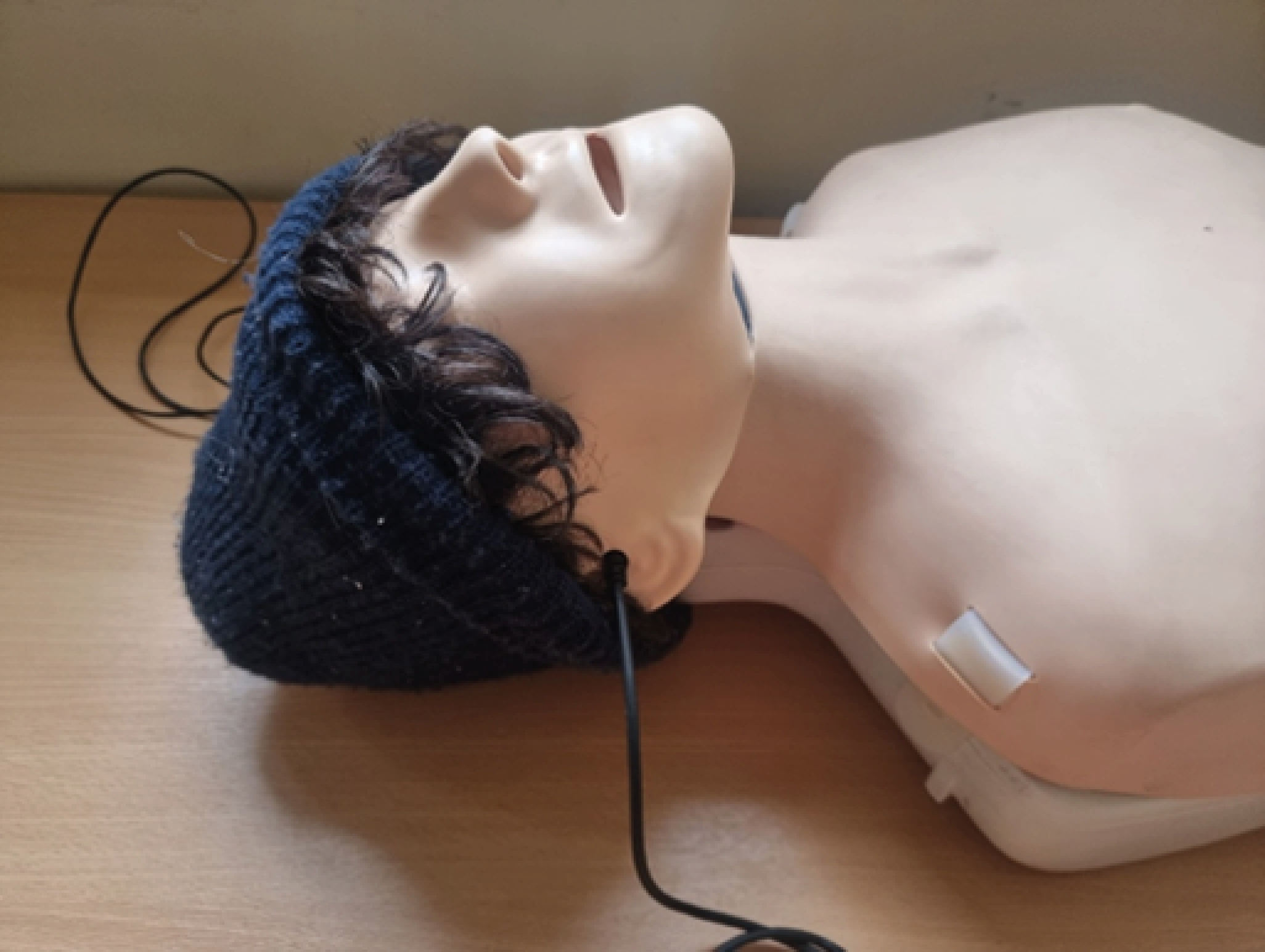
So what? The aim of this project was to incorporate the ORSIM® simulator into a manikin for use in high-fidelity simulation. A basic resuscitation training manikin was used (Figure 1). The silicone/rubber skin was removed. The ORSIM® black sensor box was placed over the head with an exit point towards the thorax (Figure 2). Polystyrene was used to support the head and cheek region (Figure 3). Inexpensive props such as hats and wigs were used (Figure 4), and patients and monitors were positioned for high-fidelity simulation (Figure 5).





We found that the ORSIM® simulator was a useful tool for training. The virtual video guidance can be used to familiarize clinicians with different pathology and improve technical skills. By incorporating the simulator into a manikin, a more realistic model can be created. Here we have used very inexpensive and often readily available equipment within a healthcare setting to achieve this. This model can be used as part of a high-fidelity simulated scenario to improve the learning experience.
1.
2.
 202 High-Fidelity Simulated Bronchoscopy: Incorporating Simulator into A Mannequin
202 High-Fidelity Simulated Bronchoscopy: Incorporating Simulator into A Mannequin
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
 Tweets
Tweets