
Simulation training sessions were designed at the University Hospital of Wales in order to implement the new national guidelines for the management of suspected haematoma following thyroid surgery [1].
Opportunities included on site portable training with a part task trainer and high-fidelity scenarios simulating patient deterioration following thyroid surgery in an immersive environment.
Our initial design for the high-fidelity set-up included a simulated neck haematoma achieved by using a second generation supraglottic airway device (SAD) with an inflatable cuff placed in the manikin’s neck with the laryngeal opening outwards and tubing inside the chest. The opening was filled with red jelly, covered by simulated strap muscles (made from simulated small bowel with interrupted sutures) and simulated neck skin (which presented a sutured incision complete with steri-strips). Ongoing bleeding was simulated by injecting liquid jelly through the SAD’s gastric port via a long connecting tube in the manikin’s thorax.
This simulation training increased confidence and familiarity with the steps required to manage post thyroid surgery haematomas in 100% (15/15) of candidates, with 73% grading the mannikin ≥4/5 for realism. However, it was costly to provide and time-consuming to set up.
It was decided to try to make the set-up cheaper and easier to reproduce without impairing quality.
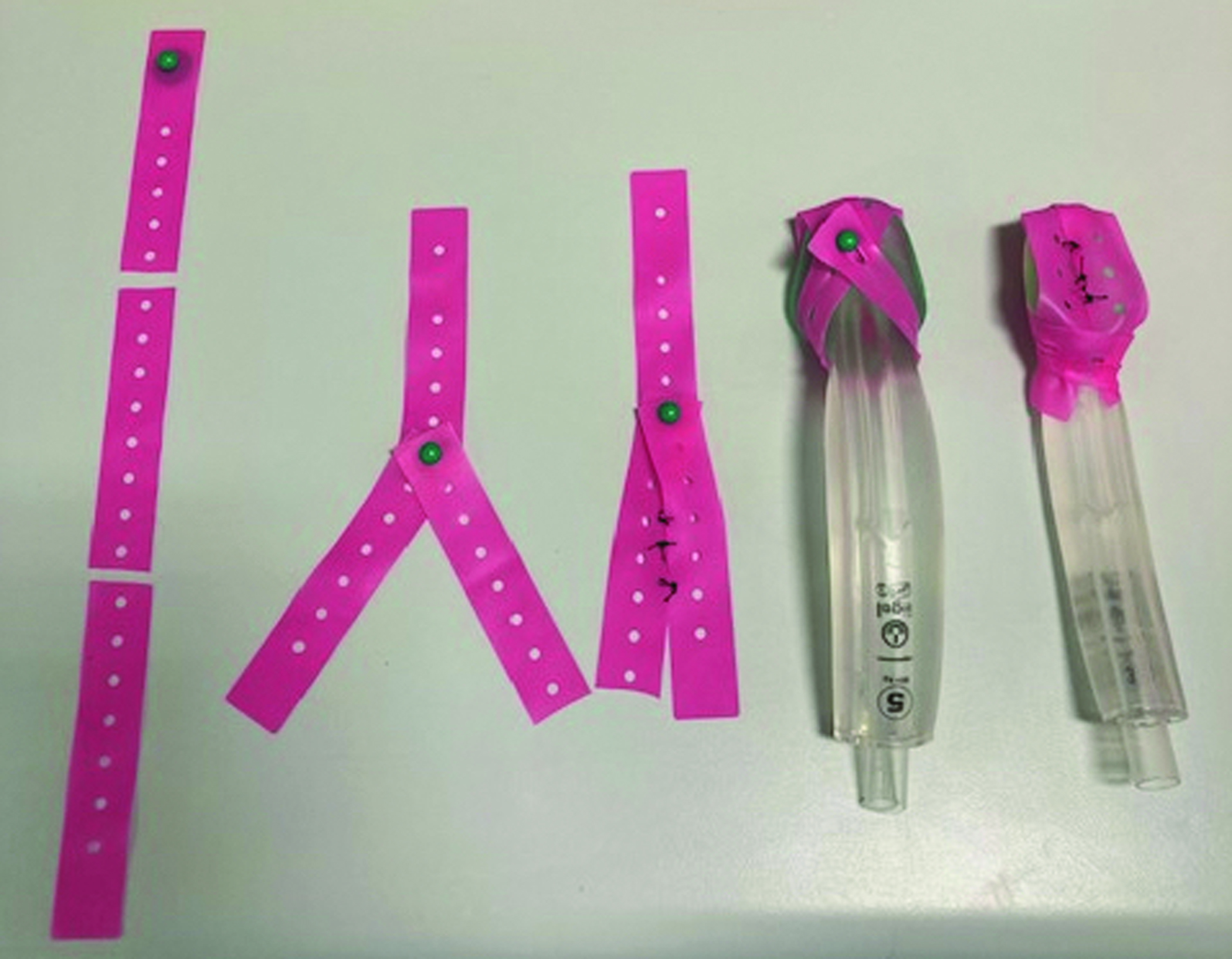
Equipment costs were reviewed and alternative options identified. Expensive components included the SAD and bowel material, which were replaced with a cheaper SAD and a disposable tourniquet fashioned as shown in Figure 1-A100. Participants used both devices and were asked for feedback.

The cost of disposable props used in each session was reduced from £133.04 to £8.52 with the new equipment. The designers also felt it was significantly more robust and easier to reproduce. This approach could also be easily adapted for mobile part-task training, improving multi-disciplinary access to training.
Feedback showed 47% of candidates felt the new set-up to be better, and 47% reported non-inferiority.
Changing to new equipment resulted in a design that was significantly cheaper, easier to source and set-up, while being at least as realistic and offering training opportunities outside the high-fidelity environment.
Authors confirm that all relevant ethical standards for research conduct and dissemination have been met. The submitting author confirms that relevant ethical approval was granted, if applicable.
1. Management of haematoma after thyroid surgery: systematic review and multidisciplinary consensus guidelines from the Difficult Airway Society, the British Association of Endocrine and Thyroid Surgeons and the British Association of Otorhinolaryngology, Head and Neck Surgery: HA, Iliff. K, El-Boghdadly. I, Ahmad. J, Davis. A, Harris. S, Khan. V, Lan-Pak-Kee. J, O’Connor. L, Powell. G, Rees. TS, Tatla; Anaesthesia 2021 Jan;77(1):82-95

 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
 Tweets
Tweets