
Kangaroo Mother Care (KMC) was introduced in the 1970s to keep premature babies warm after birth. There has been growing evidence of multiple benefits including physiological autoregulation, reduced stress, positive attachment, enhanced neurocognitive development, breastfeeding and psychological well-being. Delivery Room Cuddles (DRC) was introduced 15 years ago in Norfolk and Norwich University Hospitals as an extension of KMC. Other units have since reported the successful introduction of the process [1]. Anecdotally in our Neonatal Intensive Care Unit (NICU) parents were not routinely offered skin-to-skin contact with their infant early in their neonatal journey.
The aim of the study was to safely introduce DRC as standard practice in our NICU.
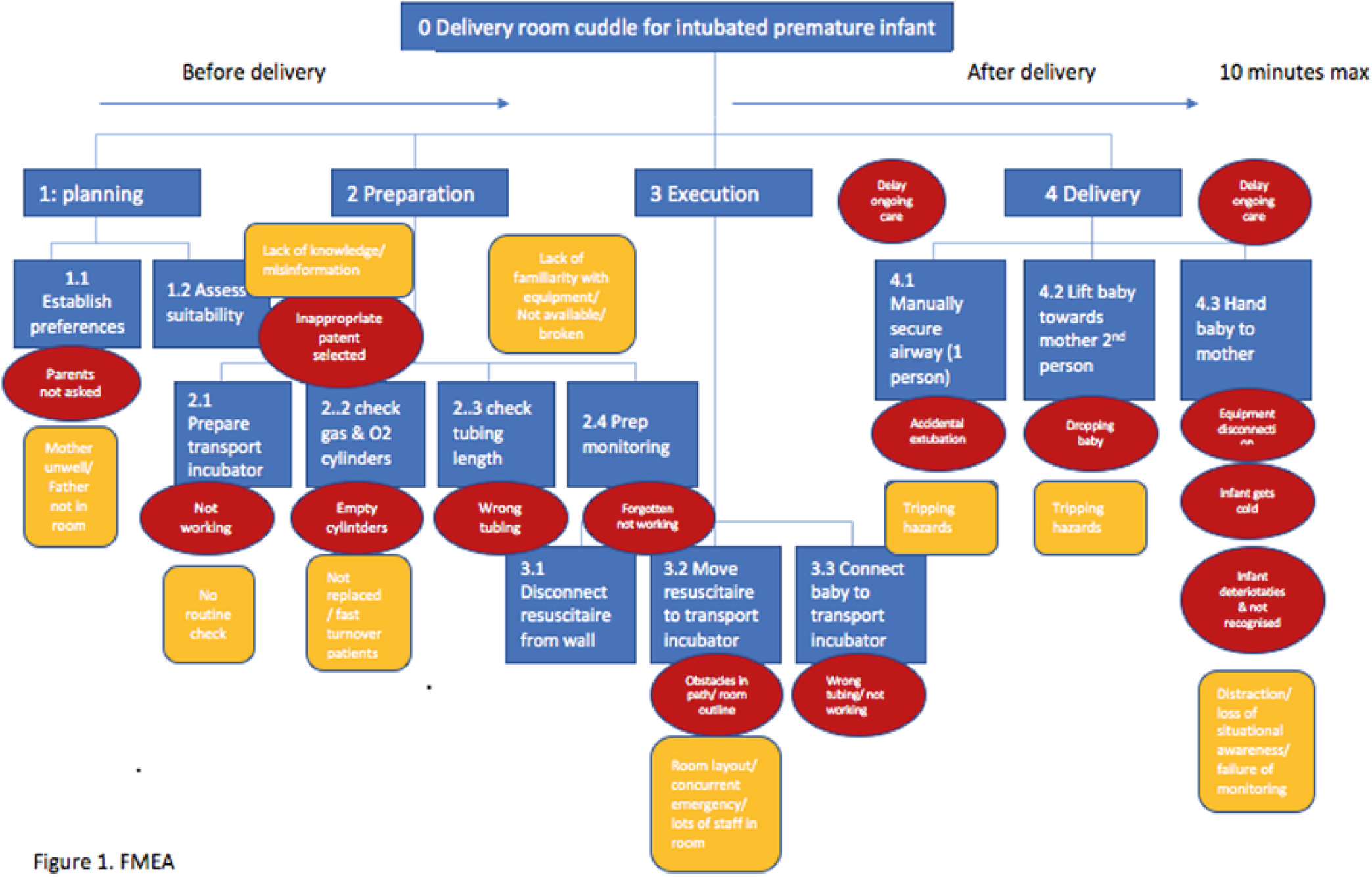
We obtained feedback on parental and staff experience with DRC. A Failure Mode and Effects Analysis (Figure 1) was then carried out to break down the DRC process into steps, highlight potential risks and mitigation strategies. Information was synthesized into a standard operating procedure (SOP) and checklist. The use of a transport incubator to mobilize premature infants was not common practice in our NICU at the start of the project; therefore, a parallel SOP was developed for this. Staff training was then carried out using a video simulation and workshops. DRC was formally introduced in April 2021 (Figure 1).

Before implementation, 54 medical and nursing staff completed the survey, rating statements on confidence from 1 ‘strongly disagree’ to 5 ‘strongly agree’. Confidence was higher in non-intubated infants 32–34 weeks’ gestation (33/54 rated 5) and lowest in intubated infants <27 weeks’ gestation (10/54 rated 5). Staff reported anxieties around equipment failure, delaying care and adverse events. Thirty-nine parents completed the questionnaire. Thirty-four babies were born locally. Only five babies had DRC, of which four had no respiratory support. Time to first skin-to-skin contact ranged from 2 hours to 17 days (mean of 5 days). DRC is becoming routine practice in our NICU with no adverse events to date. Anecdotally staff and parents report great satisfaction with DRC, although formal outcome assessment is outstanding. Introducing DRC is feasible with adequate process planning and staff training using video simulation and workshops. DRC is cherished by families, rewarding for staff and sets infants up for a positive start in the neonatal journey. With examples of successful DRC practice and emerging safety outcome data, DRC is likely to become routine practice. Using this model of process design and training, other units will also be able to safely introduce DRC.
1.
 48 Use of Simulation to Introduce Delivery Room Cuddles as Standard Practice in a Neonatal Intensive Care Unit
48 Use of Simulation to Introduce Delivery Room Cuddles as Standard Practice in a Neonatal Intensive Care Unit
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
 Tweets
Tweets