
Health Education England (HEE) provided advice on supporting simulation training during the COVID-19 pandemic, including risk assessments and personal protective equipment recommendations [1]. However, increased sickness absences [2] and withdrawal of non-clinical meetings may have hindered simulation training.
Social distancing requirements provided potential extra barriers. Locally, an emergency department (ED) staff survey (n = 60) found that 77% felt COVID-19 restrictions had impacted negatively upon simulation training, with 55% having missed a session due to limits on participant numbers intended to maintain social distancing.
HEE [1] recommended exploring video-assisted simulation, which may mitigate social distancing requirements. However, delivery can be expensive and resource-demanding. At the London Simulation Network Symposium, Gumble and Broughton [3] discussed strategies to engage remote candidates including the use of free software ‘Obs Studio’ for livestreaming.
This report documents the introduction of an in situ simulation programme utilizing Obs Studio for low-cost livestreaming.
Weekly multidisciplinary in situ simulations were organized in a UK major trauma centre ED. Faculty generally consisted of a clinical fellow (25% full-time equivalent for education) and healthcare assistant (two days per week fellowship). Specific learning outcomes and structured debriefing were used. Blog posts summarized learning for the department. Cases were organized around monthly themes and chosen to represent ED ‘core business’.
HEE funding allowed the purchase of additional equipment in 2021. An ‘observations stand’ (Figure 1) was created using a tablet computer (Lenovo Tab M10 10.1’, £110), kiosk holder (Maclocks Rise Freedom Universal Rolling Kiosk Universal Cling with Security Plate and Lock, Warsaw, Poland, £528) and ‘SimMon’ software (Castle Andersen ApS Android v1.1, £18). This could be used for ad hoc simulation with minimal faculty. One purchased webcam (Logitech Pro C920 HD, £90), a second webcam provided in-kind and a microphone (UNOOE conference microphone, £25) were connected to a laptop using a USB hub (VKUSRA 3.0, £22). Free software Obs Studio (Open Broadcaster Software v26.1.1) was used to stream two viewing angles to colleagues over Microsoft Teams (v.1.4) (Figure 2). SimMon observations were streamed via the free application ScreenStream (Agile Apps Android v1.0) and added to Obs Studio. ‘Scenes’ including observations, imaging and blood results were prepared.


The simulated observations stand. The output was controlled via the SimMon smartphone application.
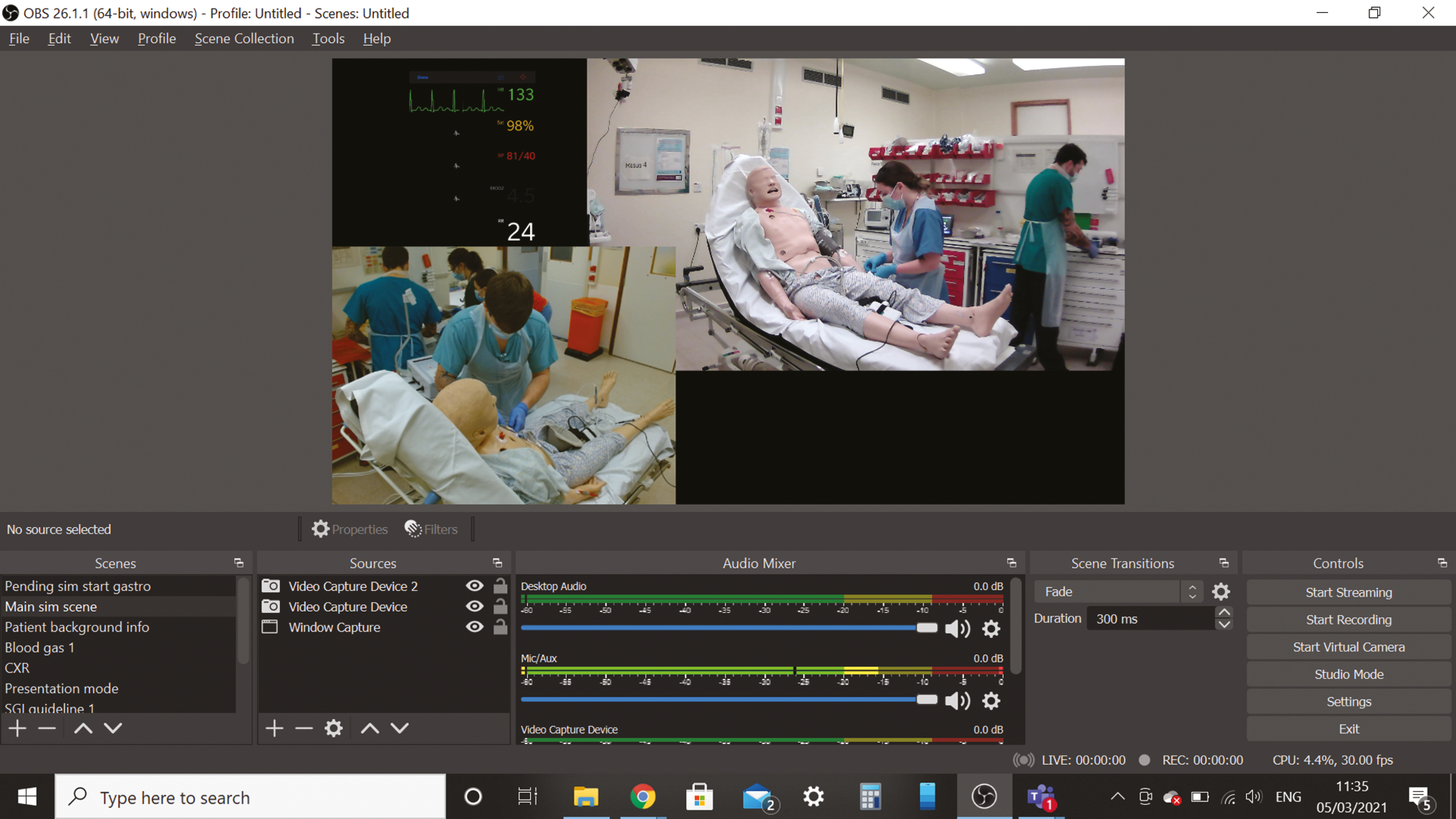
The view in Obs Studio during a simulation. ‘Scenes’ could be switched in the bottom left of the screen allowing simulated results to be shown. This view was projected using ‘VirtualCamera’ into Microsoft Teams.
Free-text feedback following sessions evaluated the teaching and any potential systems improvements. Additional surveys evaluated the impact of COVID-19 on simulation shortly after the introduction of sessions and after livestreaming began.
Between September 2020 and April 2021, at least 148 staff members physically participated across 28 simulations, plus 22 online attendees in 5 livestreamed sessions.
Free-text feedback was positive and identified potential organizational improvements. For example, one session highlighted the need to purchase additional commodes for an area of the ED, and this was actioned immediately. Feedback included:
“Great sim really useful to iron out issues with these cubicles”
“…very informative and educational. Very real”
There was a reduction in the proportion of staff reporting COVID-19 was impacting negatively upon simulation training, from 77% (November 2020, n = 60) to 34% (March 2021, n = 32). Staff missing training due to social distancing requirements reduced from 55% to 13%. Approximately, 59% of responders reported reading at least one associated blog post.
About 69% were comfortable being observed by colleagues at home versus 72% comfortable with viewers watching directly or online from an adjacent room, whilst 19% were not comfortable being watched at all. One person noted: ‘live-streaming is a big deal for junior docs and nurses… makes them more scared of joining in’.
This programme was well received and utilized by at least 170 multidisciplinary staff members. Helpful aspects were having staff with dedicated education time, senior support, funding for equipment and time/location flexibility.
Webcams, microphones and Obs Studio provided a low-cost method of livestreaming in situ with ‘scenes’ allowing remote viewers to see results, imaging and guidelines.
Livestreaming disadvantages were potentially encouraging the use of non-work time for training and performance pressure on the participants. Effective briefings including a confidentiality statement are important here for the participants’ psychological safety. These simulations were livestreamed to immediate colleagues (without recording), but there was the potential of the link being passed on. An alternative could be livestreaming to an adjacent room, although here there was little difference anticipated: 72% being comfortable with this versus 69% comfortable with viewers at home.
Adding remote aspects can increase resource demand [1]. It was possible – albeit very challenging − to run simple livestreamed scenarios with a single faculty member.
As expected, departmental crowding was a barrier to implementation. Additional funding was used to create a mobile ‘observations stand’ (Figure 1), which could facilitate opportunistic sessions at times and locations of reduced pressure.
It was possible and welcomed to run in situ simulation regularly in a busy ED. Livestreaming increased the reach of the teaching, although it had potential challenges in maintaining the psychological safety of participants. Those looking to implement similar work can view guides to in situ simulation [4] and Obs Studio [5].
The author wishes to acknowledge Laura Jacobs for her hard work facilitating the simulation sessions, the emergency medicine consultants for their support and Health Education England for providing funding to maximize our ability to carry out the effective simulation.
JK confirms sole responsibility for study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
Health Education England provided £2,422.63 in January 2021 for a combined bid by the emergency department and paediatrics department. Some of this funding was used to purchase the equipment stated in this article.
Available on request.
None declared.
None declared.
1.
2.
3.
4.
5.
 Emergency department in situ simulation during COVID-19 with low-cost livestreaming
Emergency department in situ simulation during COVID-19 with low-cost livestreaming
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
 Tweets
Tweets