
In early 2020, medical teams globally faced the challenge of preparing for an unprecedented clinical situation. As well as the predicated scale and severity of the COVID-19 pandemic clinical teams were generally inexperienced in dealing with an infectious agent of this nature. Simulation, particularly high-fidelity, plays an important role in preparing for novel, high-stakes situations. However, at this time, all clinical departments were simultaneously occupied with such preparation. This placed unprecedented demand on resource-dependant, high-fidelity simulation. Here we share our use of multiple simulation modalities, ranging from low- to high-fidelity, to prepare our multi-disciplinary obstetric theatre team for the arrival of the COVID-19 pandemic.
The aim of the study was to prepare the local team to manage COVID obstetric patients within the theatre environment, particularly in the context of obstetric emergencies. This preparation must take the form of both institutional learning (the creation of a standardized protocol specifically adapted for obstetric theatres) and individual learning (familiarity by individual team members with guidelines and their roles within them).
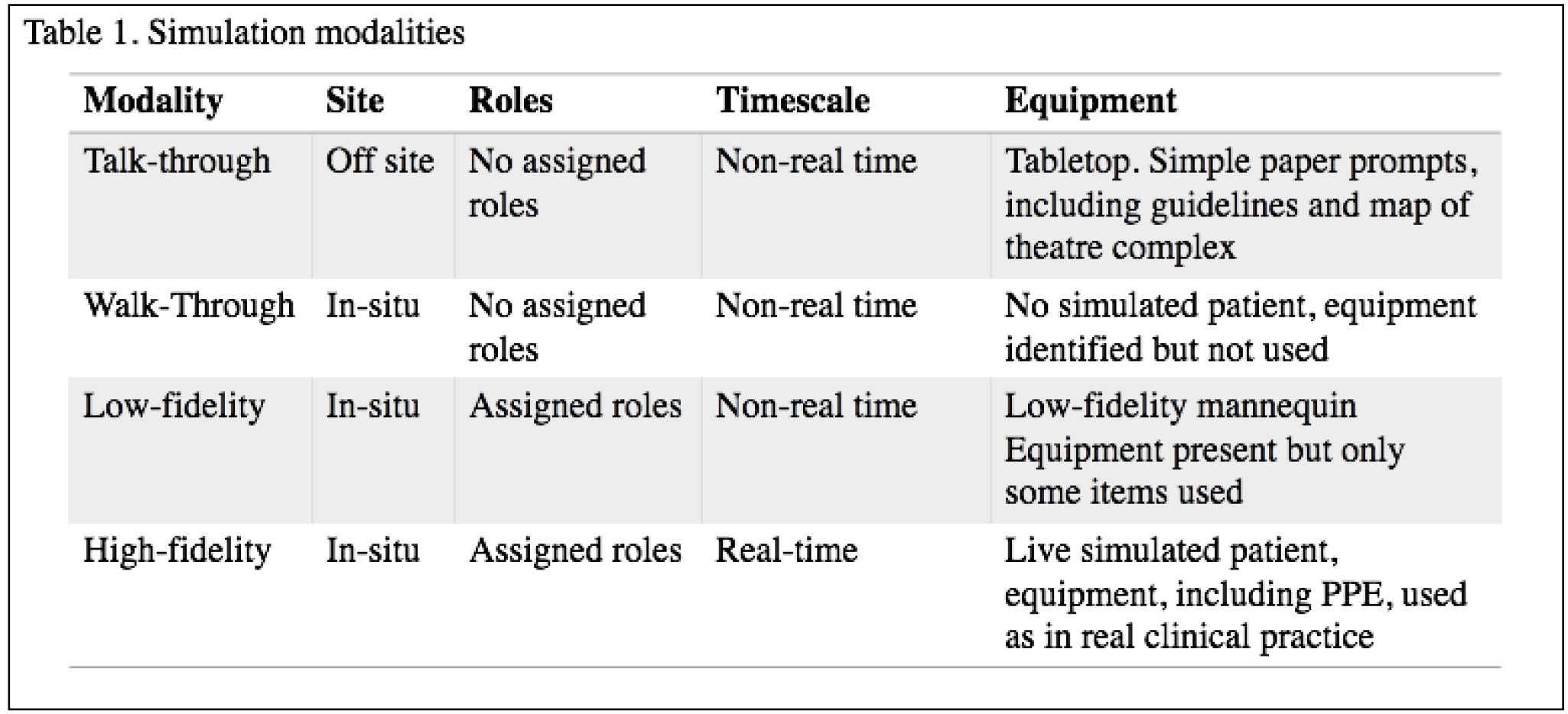
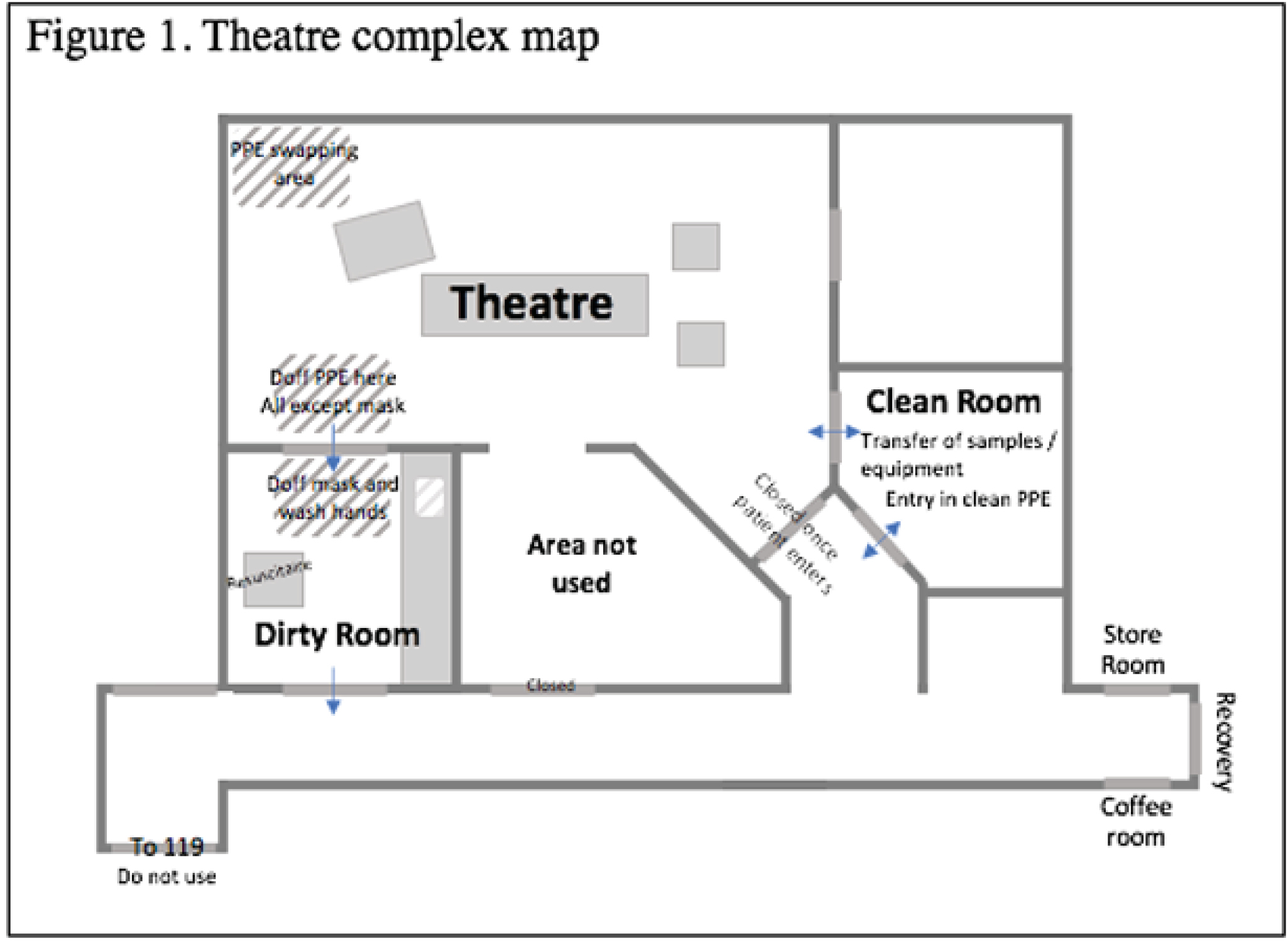
Multiple modalities of simulation were utilized (Table 1), ranging from ‘talk-through’ – table-top discussion utilizing paper prompts, such as a map of the theatre complex (Figure 1) – to high-fidelity in situ simulation. Whilst only a single high-fidelity simulation was performed, the other modalities were employed numerous times.

 |

This programme of multiple interlinked simulation modalities allowed the creation of a coherent, comprehensive and practical protocol for the management of COVID patients in obstetric theatres in advance of encountering such patients in reality. This protocol was found to be satisfactory to a group of local subject matter experts prior to the arrival of the pandemic. As management of COVID obstetric patients became more familiar, this protocol was reviewed. It was found that no significant alterations were required, indicating that, despite utilizing only a single, high-fidelity simulation session, the original programme of development had pre-empted many of the practical issues that would otherwise only have been discovered later through real-world practice. Individual learning is more challenging to define, but feedback suggested both a greater familiarity with guidelines by individual learners and was able to identify targets for more specific training (e.g. donning/doffing, definitions of aerosol-generating procedures).
High-fidelity is often viewed as the highest form of simulation for effective learning. However, its undertaking has a high resource cost. Our experience demonstrated that low-fidelity, less resource-demanding modalities provide significant benefits to both individual and institutional learning.
 176 Does High-Quality Learning Need High-Fidelity Simulation? Experience from Obstetric Theatres Preparing for the First Wave of COVID-19
176 Does High-Quality Learning Need High-Fidelity Simulation? Experience from Obstetric Theatres Preparing for the First Wave of COVID-19
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
 Tweets
Tweets