
Continuing education for cancer care providers is essential for promoting high-quality patient care. Simulation-based education can be an effective strategy to educate healthcare professionals; however, there is a lack of synthesized evidence available to inform the delivery of simulation-based education for nurses and physicians across the cancer care continuum.
This scoping review aimed to collate and synthesize the literature regarding how simulation has been reported to educate nurses and physicians about cancer care.
Scoping review following the JBI methodology. Medline, CINAHL, EMBASE and PsycINFO were searched until July 2021. Unpublished literature was searched using ResearchGate, OpenGrey and open access theses and dissertation databases. Articles were eligible if they discussed how simulation has been utilized to educate nurses and physicians about any aspect of cancer care. Two independent reviewers screened the references, extracted and analysed the data.
In total, 19 studies were included. When compared to previous reviews, our findings showed an increase in the use of virtual simulation; however, most interventions reported in-person simulation approaches and focused on improving skills (e.g. practical, communication), knowledge, confidence or decision-making for physicians and nurses caring for patients with a wide variety of cancers. Overall, simulation demonstrated positive results in educating nurses and physicians across the cancer care continuum through improved knowledge, skills and satisfaction. However, simulation interventions can be time-consuming and require significant resources for effective implementation.
Although simulation-based education demonstrated promise to educate nurses and physicians across the cancer continuum, it requires a significant allocation of resources to develop and implement these educational strategies. Educators and researchers should be aware of these challenges when planning and implementing simulation-based educational strategies.
Cancer is a major public health issue and the number one cause of death in Canada and worldwide [1]. Although lifestyle, biological and genetic factors play an important role in the risk of developing cancer, no one is exempt from the risk of this disease, and current statistics suggest a concerning increase in cancer incidence [2,3]. In 2018, the number of people living with cancer around the world was 18.1 million, and in the year 2040, this number is expected to be 29.5 million [4]. Additionally, it is expected that 44% of Canadians will develop at least one type of cancer during their lives [5].
Despite the increasing number of people living with and beyond a cancer diagnosis, these patients frequently report numerous unmet needs that can negatively affect their quality of life [6,7]. There are several complex factors associated with these unmet needs among individuals with cancer (e.g. lack of healthcare resources, healthcare professional shortage). Although many of these items are difficult to tackle, recent studies highlight one aspect in which it is feasible to intervene: educational interventions to improve the knowledge and skills of nurses and physicians, since knowledge and practice deficits among these professionals are known to contribute to the unmet needs of cancer patients [8–10]. Nurses and physicians play an important role in the delivery of cancer care, from prevention to survivorship. Although different strategies can be used for ongoing education among cancer care providers, the use of interactive educational strategies, such as simulation, has demonstrated positive results as a learning strategy for healthcare professionals [8–11].
Simulation-based education is a relatively new interactive approach, still, there is evidence that simulation can help improve knowledge, skills and satisfaction among healthcare professionals [12]. Furthermore, studies suggest that simulation-based education can be effective for most healthcare professionals, and can improve the knowledge, skills and confidence of these professionals [10,13–15]. The development of a simulation-based educational intervention usually involves planning, objectives, structure, scenario description, briefing, debriefing and evaluation, and the most common types of simulation are: (1) in-person simulation, which occurs in a simulated clinical scenario and uses life-like manikins or simulated patients to replicate clinical encounters and/or situations [16]; and (2) virtual simulation, which uses avatars, animations or video recordings of in-person simulation or virtual reality patients to replicate clinical encounters and/or situations [17–19]. Although simulation may be an applicable strategy to educate nurses and physicians on aspects of cancer care, there is a lack of synthesized and comprehensive literature on this topic to guide researchers and clinicians working in the field.
Initial searches were performed in MEDLINE, Prospero, Epistemonikos, Cochrane Database of Systematic Reviews and JBI Evidence Synthesis and no reviews nor protocols with similar topics were identified. Therefore, to better understand the use of simulation to educate nurses and physicians across the continuum of cancer care, this scoping review aims to collate and synthesize the literature on how simulation has been reported to educate nurses and physicians about cancer care.
Overarching research question: How has simulation-based education been utilized to educate nurses and physicians about cancer care?
Sub-questions: (1) What are the benefits, challenges and outcomes of the use of simulation to educate nurses and physicians about cancer care? (2) What are the costs involved in the use of simulation to educate nurses and physicians about cancer care? (3) How are briefing and debriefing strategies used during simulation-based educational strategies among nurses and physicians about cancer care?
For this review, we included nurses (registered nurses and nurse practitioners) and physicians caring for patients with cancer in any healthcare setting. Student participants alone were not eligible as we were looking for simulation strategies used to educate professionals working in clinical settings and strategies for students’ learning extends beyond the focus of this study; still, professional trainees (e.g. physician residents) that have graduated from medical, or nursing school were included. If the sample mixed nurses and physicians with other healthcare professionals, the results for nurses and physicians needed to be reported separately for the reference to be considered for inclusion.
We included studies that included simulation as an educational strategy to educate nurses and physicians in the continuum of cancer care. Simulation-based education was defined as the ‘representation of a real-life clinical experience as a model of clinical exercise to train healthcare professionals’ [20], which could be in-person simulation and/or virtual simulation (as defined above). If the simulation strategy was mixed with other educational strategies (e.g. as part of a multi-component workshop intervention), the study was only considered if the results for the simulation strategy were reported separately. Reports were also excluded if the focus of the study was on simulation modelling (representation of a physical model by a digital prototype with the intent of predicting performance), if it did not involve the use of real-life clinical scenarios, or if the simulation was used to assess skills and not as an educational strategy.
We considered studies if they reported simulation use to train nurses and/or physicians related to the care for patients with cancer (from prevention to end of life and cancer survivorship care) in any setting worldwide.
We included studies from any design (e.g. quantitative, observational, case reports, qualitative). Literature reviews alone were ineligible, but we reviewed their selection of included articles and if relevant, these references alone were included. Abstracts were initially considered, but they were only included if an associated full text could be located. Additionally, grey literature, such as theses, dissertations and research reports, were also eligible if identified in our search strategy.
This scoping review was conducted following the JBI methodology [21]. We opted for a scoping review methodology as it allowed us to collect and summarize the existing literature, using a broad research question to map the literature using a subjectivist epistemology [22]. A protocol was developed to guide this review and has been published elsewhere [20].
The search strategy was developed using keywords and controlled vocabulary with the support of two health sciences librarians. An initial search was performed in July 2021 using MEDLINE and CINAHL to identify index terms and inform the development of tailored search strategies for each database selected. After the development of search strategies tailored for each source of evidence, the following databases were searched: Medline, CINAHL, EMBASE and PsycINFO (Ovid). The search for unpublished studies and grey literature included Research Gate, OpenGrey and Open Access Theses and Dissertations. The reference lists of included reports were screened for additional studies. Reports published since 2000 and in any language were included.
The records retrieved were imported into Endnote to remove duplicates and then into Covidence® for screening. All sources were assessed against the inclusion criteria by two independent reviewers (AS, CH and/or KT) first by title and abstract, and later at the full-text level; conflicts were solved through discussions among the reviewers or with the input of a third reviewer (ML).
Data were extracted by the first author (AS) and checked by a second reviewer (CH or KT) using a data extraction tool that was developed and pilot-tested for this study. This data extraction tool included aspects related to study characteristics, population, concept, context and other key aspects relevant to our review. The data extracted was assessed using an inductive content analysis approach and numerical frequency counts, and the results are presented using a tabular form and a narrative summary to describe how simulation has been reported to educate nurses and physicians about cancer care. In line with the JBI scoping review methodology, a quality appraisal of the included literature was not conducted, as our intent was to map the literature with a broad lens and not provide guidance to practice [23].
The searching process yielded 4047 reports, and after duplicates were removed, we had a total of 3076 references that were assessed by title and abstract, resulting in 270 references being assessed at the full-text level and a total of 19 references that were included in this review. For details on the searching process and study selection please refer to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) Extension for Scoping Reviews flow chart in Figure 1.

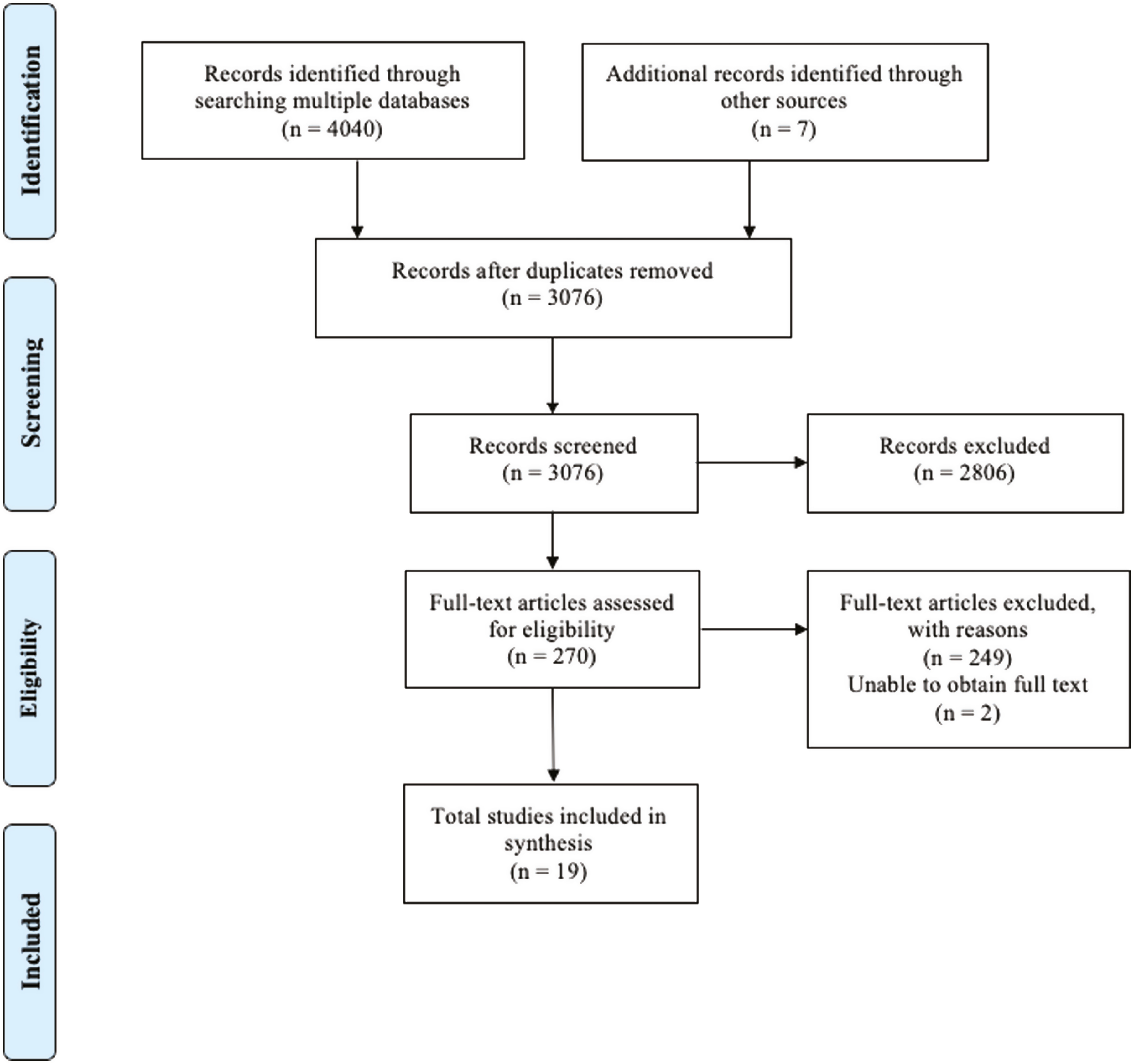
Preferred Reporting Items for Systematic Reviews and Meta-analyses Extension for Scoping Reviews flow chart.
From the 19 reports included in this review, the majority were written in English (n = 18), from the United States (n = 11), published from 2016 to 2021 (n = 13) and included a pre-test post-test design (n = 15). Additionally, most studies were focused on the following aspects of the cancer continuum care: treatment (n = 7), adverse medical events (n = 4), screening and diagnosis (n = 3), diagnosis (n = 3) and palliative or end-of-life care (n = 2), while no studies on survivorship care were found in the literature. Details related to the main characteristics and findings from the included studies can be found in Table 1.

| Author, year, country | Objective | Sample | Outcome measures | Major findings |
|---|---|---|---|---|
| Andrade et al. (2010), USA [24] | To study the feasibility of creating standardized patient avatars in a virtual world for training medical trainees to deliver bad news | Ten medical trainees (5 first-year clinical geriatric medicine fellows and 5 internal medicine postgraduate year 1) | Self-efficacy affective competency score (ACS, maximum score = 30); Witmer’s Presence Questionnaire; Modified Breaking Bad News Assessment Schedule (BAS) | Self-efficacy (ACS) scores improved overall: before, 20 ± 4, versus after, 24 ± 3, p = 0.001 Participants (all) considered the experience positive and novel, yet they mentioned that avatars were not able to portray body language cues. |
| Arnaoutakis et al. (2016), USA [25] | To examine haematology/oncology trainees’ perceptions about the value of and techniques used for simulations of specialty-specific, essential conversations with patients and families, and debriefing sessions that followed | Seven medical fellows (first-year haematology/oncology) | Facilitators used the Performance Enhancement through Augmented Reflective Learning (PEARLS) debriefing method to access participants’ reactions, performance and behaviours | The curriculum was highly effective and positive for learners’ experiences. The intervention also confirmed the feasibility for implementing a simulation-based communications program in a mid-sized haematology/oncology program. |
| Askew et al. (2012), USA [26] | To describe a nursing simulation exercise program within a surgical oncology unit to prevent adverse events/failure to rescue among oncology patients | Forty-five oncology nurses | Observational data; quality improvement indicators | There was no failure to rescue in the year following the program, cardiac and respiratory arrest decreased by 300% and emergency response team events increased by 60%. Nurses also expressed more confidence, knowledge and skills after the exercise. |
| Aubin-Auger et al. (2013), France [27] | To develop a training course to enhance general practitioners’ communication skills in colorectal cancer screening, based on the two previous qualitative studies. | Eighteen general practitioners | Program development | A two-sequence training program was built, including role-playing and presentation of the video followed by a discussion. An RCT (reference below) [28] is being conducted to evaluate the efficiency of the program. |
| Aubin-Auger et al. (2016), France [28] | To test if the implementation of a training course focused on communication skills among general practitioners would increase the delivery of guaiac faecal occult blood test and colorectal cancer screening participation among the target population of each participating general practitioner | Forty-five general practitioners (17 in the intervention group and 28 in the control group) | Colorectal cancer screening rates over 7 months; the number of practitioners reaching a patient participation rate of 65%; the number of practitioners reaching a participation rate of 45%; the number of guaiac faecal occult blood tests delivered by practitioners | The educational program was effective at increasing patient participation (the rate per GP was 36.7 in the intervention group and 24.5 in the control group), patient-centred care and giving practitioners the skills to motivate non-compliant patients appeared to increase colorectal cancer screening participation rates. Using patient-centred care and giving GPs the skills to motivate non-compliant patients appeared to be good ways to increase their CRC screening participation rate, still, participation rates have remained low. |
| Deluche et al. (2020), France [29] | To relate the implementation of simulation as a teaching tool to the consultation announcement (e.g. diagnosis disclosure, cessation of treatment). The other objectives are the evaluation of the necessary skills of the learner to carry out a consultation announcement, their evolution over time and the measurement of learner satisfaction | Fourteen interns (residents from the medical oncology and radiotherapy departments) | Skills assessment and development were measured using the Likert scale comprising four levels and grouped into three skill categories (verbal, felt and relational) | All residents felt stressed before a consultation. Skills improved following simulation for all criteria, particularly for adaptation to patient reactions, use of appropriate vocabulary and reduction of stress. Most students were ready to repeat this type of training. |
| Dietrich et al. (2021), France [30] | To investigate the utility of simulation for disclosing a melanoma diagnosis | Fifteen dermatology residents | Physician satisfaction and perceptions about benefits and assistance in their practice. | The majority of participants thought the session improved their communication skills, attitude, and control, and helped with stress management. They rated the usefulness of the simulation at 7.79/10 on average. |
| Henselmans et al. (2019), Netherlands [31] | To examine the effect of shared decision-making training for medical oncologists on observed shared decision-making in standardized patient assessments | Thirty-one oncologists (15 intervention and 16 control groups) | To write a treatment plan, how realistic and how comparable to their clinical practice the simulated consultation was; Observing Patient Involvement scale (OPTION12); Observed shared decision-making was assessed with the 4 shared decision-making; observed communication skills; 5-item Patient Satisfaction Questionnaire | The training had a significant effect on observed shared decision-making in the simulated consultations and improved observed behaviours. The training also improved oncologists’ information provision skills, skills related to anticipating/responding to emotions, and their satisfaction. |
| Huang et al. (2021), Taiwan [32] | To evaluate the effect of virtual reality-based training including the thinking-path tracking map method, virtual reality simulations and bedside assignments on nurses’ familiarity, confidence and anxiety regarding treatment decisions and treatment-related knowledge/skills | Twenty-six nurses in an oral cancer ward in Taiwan | Pre-test survey (baseline self-efficacy) and post-test survey (self-efficacy and satisfaction) | The training significantly increased nurses’ (1) familiarity and confidence regarding knowledge of treatments and treatment decisions, and (2) confidence in their skills in bedside pre-treatment education for admitted oral cancer patients. |
| James et al. (2016), USA [33] | To develop interprofessional team training opportunities using simulated cancer care scenarios to enhance collaborative practice skills within clinical oncology | Twenty-three oncology fellows and nurses | Observations; peer-to-peer assessment of team performance; post-programme survey | The simulation scenarios were successfully implemented and participants valued the experience and indicated that they acquired new knowledge, skills and attitudes to enhance interprofessional collaboration in cancer care. |
| Kubal et al. (2016), USA [34] | To examine whether a measurement and feedback system led to improvements in adherence to clinical pathways in breast, lung and gastrointestinal cancers | Forty-eight providers (composed of medical oncologists, radiation oncologists, surgeons and advanced practice providers) | Observational scores of each vignette within each domain (history, physical, workup and diagnosis with treatment plan, maximum score 100%) – 3 measures in 9 months | The training increased pathway adherence between the third and first rounds of data collection particularly. Breast improved by 13.6% and lungs improved by 12.1% over baseline, while gastrointestinal decreased by 1.4% |
| Kuhrik et al. (2008), USA [35] | To share insights, experiences and lessons learned regarding the development and implementation of a simulation program for oncology nurses to assess early clinical manifestations of oncologic emergencies, establish priorities, make decisions and take action and work effectively as a team | Eleven registered nurses in an oncology clinical practice setting | Observation; program evaluation | The nursing participants agreed the simulation laboratory was the preferred place to practice skills and learn from their mistakes. |
| Page (2016), USA [36] | To assess the effectiveness of a quality improvement intervention designed to reduce central line-associated bloodstream infections rates in the oncology inpatient unit, using a simulation-based educational intervention for oncology nurses | Twenty oncology nurses | Pre-test/post-test survey to identify knowledge regarding central line access, care and maintenance techniques on the simulation task trainer | The educational program increased 16.9% of the nursing staff’s competence related to the care and maintenance of central lines. The rate of central line-associated bloodstream infections decreased from 5.86 per 1000 patient line–days to 3.43 6-months post-intervention. |
| Schulz et al. (2019), Germany [37] | To evaluate the advantages and limitations of the novel uro-trainer (UT) concerning training for transurethral resection of bladder tumours | Twenty-two urological physicians, including residents and consultants | Realism; self-assessment of key competencies for the correct and safe completion of transurethral resection of bladder tumours (TUR-BT) at the end of the training | A total of 27.3% of the participants had already experienced overtaxing situations during TUR-BT and only a few reported high satisfaction with the classical teaching model. Consultants achieved significantly higher overall scores and safety and visualization subscores. The self-assessed capability to perform a TUR-BT was correlated with overall UT scores. Participants indicated improvements in several procedural skills and overall benefit of the training; UT was rated 4.6 on a 5-point scale by consultants (limitations included tissue feedback and authenticity of different tissue layers). |
| Taunk et al. (2021), USA [38] | To analyse if virtual reality-based intracavitary brachytherapy simulation will improve residents’ confidence, engagement and proficiency | Fourteen resident physicians (including five postgraduate years [PGY] 2, three PGY 3, four PGY 4 and two PGY 5) | Self-Confidence Scale; Procedural Steps; Resident Familiarity with Procedure; Survey of Learning Experience; Perceived Learning Usefulness; Usability and Flow | The simulation improved resident confidence (1.43–3.36), and subjective technical skill in assembly (1.57–3.50) and insertion (1.64–3.21), considering a 5-point scale; decreased the average time of implant from 5:51 to 3:34 and median technical proficiencies increased from 4/5 to 5/5. Residents found the simulation a useful learning tool and indicated an increased willingness to perform the procedure again. |
| Vioral (2014), USA [39] | To determine if oncology nurses’ use of simulated electronic learning vignettes increased their knowledge of the American Society of Clinical Oncology and the Oncology Nursing Society chemotherapy safety standards, as well as oncology nurses’ satisfaction with the simulated electronic learning vignettes | Sixty-six chemotherapy-competent RNs | Learning management system scores and satisfaction. The oncology nurses’ knowledge was reassessed 4 weeks after the education to measure knowledge retention. | Knowledge of chemotherapy errors initially improved but returned to baseline after one month. Participants were more satisfied with the content than with the delivery and system methods. |
| Wayman et al. (2007), USA [40] | To investigate the effects of medical error disclosure training in a simulated setting for paediatric oncology nurses | Sixteen oncology nurses (paediatric) | Perceived self-efficacy in communication; the extent to which training evoked their ‘true’ verbal and non-verbal skills; Perceived Fidelity Index; internal validity was measured using two assessments for effectiveness | The training increased nurses’ communication self-efficacy to carry out medical disclosure, and ratings of setting realism and simulation effectiveness were high (21 out of 25 composite scores). The fidelity or realism of the simulation ratings was significantly related to three study measures (self-efficacy, component effectiveness, and overall effectiveness). |
| Weston et al. (2018), USA [41] | To assess family nurse practitioner students’ (FNPs) and family medicine residents’ (FMRs) baseline knowledge of breast and cervical cancer risk factors to inform curriculum needs and to determine the impact of a high-quality interprofessional education simulation on self-reported confidence in counselling women reluctant to engage in breast and cervical cancer screening or evaluation | Seventy-six family nurse practitioners students and family medicine residents | Survey of risk factors for breast or cervical cancer; faculty observed shared values, mutual respect and role utilization during the simulation; standardized patients reported on team interaction and perceptions of receiving patient-centred care; pre-post confidence survey in performing the procedure | Following the simulation, debrief feedback findings suggest improved attitudes toward collegiality, communication and understanding of other interprofessional roles among both disciplines and confidence in counselling women reluctant to have breast or cervical cancer screening improved across both disciplines. Overall, the average risk factor knowledge score was 8.5 points out of 12 points for breast cancer (70.4%), and 7.8 out of 12 points for cervical cancer (65%). The highest change in confidence for both groups was in counselling a woman with an abnormal result after a mammogram (62.5% increase for FNP and 48.9% for FMRs). |
| Wu et al. (2020), Taiwan [42] | To train nurses on how to equip oral cancer patients with self-care skills by enhancing their knowledge of treatments according to clinical staging, and the patients were satisfied with the nurses’ pre-treatment educational services | Seventeen primary care nurses | Nurses’ treatment decision-making knowledge was assessed by completing an assignment of charting the treatment decision plan for each patient (which included all treatment choices for different cancer stages) | Following this project, an increase in nurses’ knowledge about treatment decisions, familiarity with newly developed educational aids, and confidence in providing educational services to admitted oral cancer patients were observed. A high number (88–95%) of nurses reported that they that educational aids increased the effectiveness of bedside pre-treatment service, and that they are willing to recommend it to their peers. |
Following the inductive content analysis approach, we grouped our findings into five categories to address the aim of this review: (1) the clinical scenarios and purpose of the simulation; (2) the simulation methods; (3) costs involved in the use of simulation-based education; (4) the use of briefing and debriefing; and (5) simulation outcomes, challenges and benefits.
The focus of the use of simulation was diverse in the literature and studies were focused on teaching practical skills (e.g. chemotherapy administration, transurethral resection) (n = 7) [26,32–34,36–38]; communication skills (n = 5) [24,25,27,30,40]; both practical and communication skills (n = 2) [28,29]; knowledge and/or confidence (n = 3) [39,41,42]; and decision-making (n = 2) [31,35]. Regarding the emphasis on the clinical scenarios in the literature, the types of cancer included colorectal (n = 2) [27,28], oral (n = 2) [32,42], breast (n = 1) [24], breast and lung (n = 1) [25], breast, lung and GI (n = 1) [34], breast and cervical (n = 1) [41], lung (n = 1) [26], melanoma (n = 1) [30], gastric and oesophageal (n = 1) [31], bladder (n = 1) [37] and cervical (n = 1) [38]. Some studies had a generic focus and did not specify the cancer type (n = 6) [29,33,35,36,39,40]. Although the participants of the simulation were similar in proportion, the majority were physicians (n = 10) [24,25,27–31,34,37,38], followed by nurses (n = 8) [26,32,33,35,36,39,40,42], and both (n = 1) [41].
A variety of simulation methods were identified, and the majority included in-person simulation (n = 10) [25,26,29–31,33,35,36,40,41], followed by virtual simulation (n = 9) [24,27,28,32,34,37–39,42]. Additionally, of the articles that used in-person simulation design, most of them reported simulated patients (e.g. trained professionals or actors) (n = 7) [25,29–31,33,40,41], followed by mannequins (n = 1) [35] and a central line simulation task trainer (n = 1) [36]. One article did not specify this aspect of the intervention [26]. With respect to virtual simulation, most articles included either avatars or vignettes (n = 6) [24,32,34,37,39,42], followed by records from real-life scenarios with simulated patients (n = 3) [27,28,38].
Most articles did not describe the cost of the simulation intervention used, with only four authors discussing this aspect. Arnaoutakis et al. [25] reported in-person simulation with simulated patients and reported a cost of $175 (USD) per fellow (including the fee for the simulated patient, and there was no fee for using the institutional simulation laboratory). Kuhrik et al. [35] mentioned costs involved in simulation in their literature review but did not specify this in their intervention. While Schulz et al. [37] mentioned that virtual simulators are associated with high-cost acquisition, Taunk et al. [38] mentioned that virtual reality was low cost, but neither article specified monetary values.
Debriefing following simulation is considered an important part of simulation-based education and it can be a fundamental aspect influencing simulation effectiveness. Debriefing provides participants with the opportunity to engage in reflecting on their simulation experience and performance to enhance their learning process [43]. Also, there are different types of debriefing activities (e.g. facilitator-guided, self-guided) and these can occur during the simulation activity, immediately after or days after the simulation [1,2]. Of the studies included in this review, most mentioned using a debriefing activity, and the main purpose behind the debriefing was to obtain and provide constructive feedback (n = 8) [24,25,29,30,33,35,40,41] or to use its results to develop a personalized educational plan (n = 1) [26]. One study described a debriefing activity without explicitly labelling it as such [34], and the remaining studies did not mention debriefing activities at all (n = 9) [27,28,31,32,36–39,42]. Additionally, some authors analysed the data from the debriefing qualitatively to better understand the impact of their intervention [24,25,30,41], while others [25,40] asked participants about their perceptions of the debriefing, and most participants reported that the activity was helpful and effective.
Simulation activities also usually include an orientation or even sharing of materials beforehand to ensure that the learning is successful, which is often called briefing; although only two authors specifically mentioned the use of briefing activities [29,30], all authors (directly or indirectly) mentioned providing informational resources before the simulation activity.
In this review, we defined as outcomes any measurement reported to explore the actual or potential effects of simulation as an educational strategy to improve cancer care provided by nurses and physicians (e.g. knowledge and confidence). Details regarding the methods included to measure outcomes, as well as specific results from each of the included studies, can be found in Table 1.
Overall, authors who measured outcomes from the simulation highlighted that the intervention improved self-efficacy [24,40], knowledge [26,32,33,35,39,42], confidence [26,32,38,41,42], satisfaction [30,31], decision-making process [31], attitudes [30,33] and stress levels [29,30]. Additionally, the simulation had a positive impact on the skills (either practical or communication) [25,26,28–31,33–35,37,38,41], competence [36], performance [31,34], team dynamics [33,41], as well as pathway adherence [34] and quality indicators [26,36]. Some authors also considered simulation-based education feasible [25], effective [25,28,33,40,42] and useful [30]; and participants perceived the intervention as a positive [24,25,32], beneficial [30], engaging [38], realistic [40,41], non-threatening [35,37] and novel [24,39] experience and were generally satisfied with the learning model [39,42]. Although the study from Aubin-Auger et al. [28] reported that simulation can be a good way to educate healthcare professionals and improve colorectal cancer screening participation, participation rates remained lower than the ideal among participants from that study.
Despite the observed benefits of simulation-based education, there were also several challenges mentioned related to the simulation use and outcome measures. Some authors mentioned limitations related to the simulation methods included, such as difficulties in observing non-verbal clues in avatars [24], lack of physical responses of mannikins [35], tissue feedback and authenticity of different tissue layers [37] and some participants were not familiar with the technology or equipment, making the learning process more difficult [38,39]. Also, there were reports on the challenges in the administration of the simulation; for example, when participants were experienced practitioners, it was difficult for facilitators to modify the scenario in a timely manner during the simulation [35]. Time constraint issues made it difficult for some providers to participate in the training [27,28,39], as well as some participants reported difficulties to perform the simulation within the timeframe stipulated [29,36].
Authors also mentioned that it was difficult to control potential confounders in the results (e.g. participants may have been exposed to other interventions over time, patients may have received other optimal care not related to the simulation, and complexity involved in clinical pathways and cancer types) [26,34,36,39,40], as well as differences in the baseline scores between control and intervention group [31]. Lastly, other challenges included participants’ resistance to change [36], resources involved in developing and implementing the simulation [36,38] and costs [37,38]; some authors did not mention specific challenges in simulation use [25,30,32,33,41,42].
This scoping review synthesized how simulation-based educational strategies have been utilized to educate nurses and physicians across the continuum of cancer care through a literature review of the 19 selected articles that have been published worldwide on this topic. The studies selected included different outcomes to measure the impact of simulation, and most of them had a small sample size, which limits the transferability of results into different healthcare contexts. Still, findings from this review brought forward evidence that simulation-based education can be an effective learning strategy to teach oncology nurses and physicians, as all studies that measured outcomes from the simulation stated positive impacts on the learning process through improving measures from baseline. Also, the complexity involved in the different pathways and cancer types was highlighted as a challenge for educators developing and implementing simulation-based educational interventions in the field [34].
Although authors predominantly reported in-person simulation [25,26,29–31,33,35,36,40,41] over virtual simulation [24,27,28,32,34,37–39,42], the difference was relatively small (10 in-person over 9 virtual) when compared to a previous review [10] published in a similar topic that investigated simulation use in the continuum cancer care among nursing professionals and students (10 in-person over 2 virtual). This potential growth in virtual simulation use may be attributed to growing interest in virtual learning strategies. This became particularly relevant in supporting healthcare professional education during the COVID-19 pandemic, in light of public health measures to reduce viral spread that directly impacted the learning process of many health professionals [44,45].
Despite several benefits of the use of simulation-based education for cancer care providers (e.g. improvement in skills and knowledge), the studies included in this review also reported several challenges in the application of the intervention. These limitations included challenges in the use of mannikins or avatars (e.g. lack of response/reality) [24,35,37], and in learner participation (e.g. lack of time, unfamiliarity with technologies and resistance to change) [27–29,36,38,39]. Simulation-based education, despite its potential effectiveness, can also be very time-consuming. Given the evidence that training for busy healthcare professionals may contribute to the incidence of work-related issues (e.g. burnout) [46], educators need to be mindful of this aspect while planning simulation activities for cancer care providers.
Additionally, debriefing activities were highlighted in the literature as an important aspect of the learning process of simulation-based educational strategies; these findings are similar to what authors [43] from another review investigating the effectiveness of debriefing methods have found, as all the studies included in that review stated that debriefing had positive benefits, and this was an important aspect for the learning process. That may be because debriefing activities support the learning process through self-reflection of the simulation activity, allowing the learner to critically think about their performance and ways to improve their practice [43].
Lastly, simulation-based educational activities can involve relatively high use of resources (e.g. equipment and personnel) and costs, which was highlighted in the literature as a potential implementation challenge [ 36–38]. Previous authors, outside of this scoping review, who conducted cost-utility analysis in the use of simulation found that healthcare simulation activities costs can vary between $15 and $1900 (USD) [47]; when comparing virtual with in-person simulation, virtual simulation was more cost-efficient, with a cost of $10.89 (USD) per participant compared to $36.55 (USD) per participant in in-person simulation [48]. Thus, virtual simulation may be an option to help to minimize costs and improve the feasibility of simulation-based educational strategies [49].
Findings from this review can be used to guide educators and researchers planning to develop, test and/or implement simulation-based education, in cancer care and beyond. Results from this scoping review will guide the development and testing of a simulation-based educational strategy aimed at improving nursing and physicians’ assistance to cancer patients through a pilot mixed-methods study.
Following the current methodological guidance for scoping reviews, we did not perform a quality appraisal of included studies, which is congruent with our aims but also limits the applicability of our results. Moreover, scoping reviews are exploratory by nature and our results do not intend to provide direct guidance to practice. Although studies included reported several outcomes, none of them reported the actual impact of simulation use on the quality of care received, nor on the quality of life of patients. Lastly, the inclusion criteria for this review were very specific and may have omitted the inclusion of articles that could somehow be potentially relevant to the topic, such as studies conducted with other cancer care providers beyond nurses and physicians.
Simulation-based education demonstrated positive results in the literature as an educational strategy for improving knowledge, skills and satisfaction among nurses and physicians across the continuum of cancer care. When compared to previous reviews, our findings show an increase in the use of virtual simulation, although the majority of studies still predominantly included in-person simulation. Nevertheless, simulation interventions can be time-consuming and require vast resources (e.g. equipment, costs, personnel) for effective implementation; educators and researchers should be aware of these challenges when planning simulation-based educational strategies. Despite the potential challenges associated with the use of simulation, this educational strategy was highlighted as positive for the learning process of oncology nurses and physicians. As well, virtual simulation may be an option to improve the feasibility of simulation-based educational strategies by minimizing costs while increasing the accessibility to large groups of clinicians located in geographically diverse and remote locations. High-quality continuing education for these health professionals should be considered an ethical imperative for cancer care systems as a potential strategy to improve healthcare delivery and patient care.
All authors contributed to the study’s conception and design. Material preparation, data collection and analysis were performed by AS, KT and CH, with the support of JG, KW and MLF. The first draft of the manuscript was written by AS and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
This scoping review is part of a PhD thesis research study funded by a Canadian Association of Nurses in Oncology (CANO) Research Grant; a Canadian Alliance of Nurses Educators using Simulation (CAN-Sim) PhD student award; and an International Nursing Association for Clinical Simulation and Learning (INACSL) Debra Spunt Research Grant.
The data supporting the findings of this study are available within the article.
Not applicable.
The authors have no relevant financial or non-financial interests to disclose.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
 The use of simulation-based education in cancer care: a scoping review
The use of simulation-based education in cancer care: a scoping review
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets