
High-fidelity medical simulations can help students successfully navigate the stressors of medical training and practice. Because sufficiently high stress levels can interfere with learning, the balance of stress and resilience factors during simulation training should be carefully curated. However, student experiences of stress and resilience during high-fidelity simulations are seldom well characterized, especially in military medical training. With this in mind, the authors investigated students’ lived experiences of stress and resilience during a well-established high-fidelity simulation at a military medical school.
Fourth-year active-duty military medical students (n = 23) from the United States Air Force, Army, and Navy who were attending Operation Bushmaster – a 5-day, high-fidelity military medical simulation – were interviewed during and after the simulation. Data were analyzed via a hermeneutic phenomenological qualitative approach. Another 21 students reported their stress levels and trait mindfulness. Experts rated their performance at Operation Bushmaster.
Participant narratives pointed towards major internal stressors, including chronic uncertainty and fluctuating motivation, and external stressors, such as weather and equipment-related challenges. Narratives also identified multiple factors that mitigated stress, including the use of mindfulness skills (especially mindful/tactical breathing), giving/receiving social support, shifting perspectives to centre connections between Operation Bushmaster and students’ professional purpose, and positive self-talk that gave participants permission to make mistakes and learn from them. There was a moderate positive correlation between mindfulness and performance at Operation Bushmaster.
These stress and resilience factors are critical leverage points for educators seeking to optimize learning during Operation Bushmaster and other high-fidelity simulation trainings. Future research should continue to examine how the balance of these factors impacts medical students’ immediate learning (e.g. regarding medical decision-making, skill and leadership) and longer-term ability to successfully navigate the stressors of the medical profession.
Medical training and practice are stressful. Both feature long hours, times of limited sleep quality or duration, exposure to patient death and suffering, and frequent demands to demonstrate knowledge and skills in high-stakes, time-pressured settings [1]. Sufficiently high stress levels foster poor mental health, alter decision-making[2] and impair basic cognitive operations – such as processing speed, attentional control and working memory [3,4] – that are likely essential for medical cognition and care. Medical students and early-career physicians may be especially vulnerable to these effects of stress because they have had less time to routinize job role demands and learn effective coping strategies tailored to them and their job role [1]. Recognizing this, medical schools have increasingly relied on simulation-based training to prepare students to successfully navigate the stressors of their profession [3,5]. Many of these simulations involve purposeful, time-limited exposure to elevated stress. While these approaches are promising, the level of stress students experience must be carefully curated. Too much stress interferes with physiological components of learning, like long-term potentiation [6], and increases the risk of burnout and poor mental health [5]. Stress can thus impede the very growth in thought patterns and behavioural repertoire that these interventions were meant to promote. It is, therefore, critical to understand student experiences of stress during medical simulations and identify resilience factors that could help students moderate stress and maximally benefit from the experience.
Previous research suggests several factors can help medical students remain resilient against stress during simulation-based training. For example, mindfulness – paying attention to the present moment, on purpose, in a non-judgemental manner[7] – reduces psychological distress among medical students[8] and correlates with better performance when they treat simulated life-threatening conditions [9]. Social support and connectedness have also been implicated in resilience among medical students and professionals [10,11]. Effective military trainings suggest that realistic positivity in communication and a culture of giving/receiving aid are key aspects of team environments that foster resilience [12]. Compassionate self-talk that gives learners permission to err is also linked to increased resilience [13]. Finally, shifting perspectives by connecting present adversity to a valued purpose is likely to increase resilience among medical students [10]. Indeed, one long-standing medical school programme that encouraged students to find meaning and purpose in their work achieved over 75% reductions in mental health symptoms [14].
With this previous research and the need to better understand medical students’ lived experiences of stress and resilience during simulation in mind, we conducted a qualitative investigation and a quantitative pilot study of fourth-year students attending Operation Bushmaster, an annual 5-day military medical simulation. Operation Bushmaster is both the culminating evaluation of the Uniformed Services University’s military-unique curriculum and a high-fidelity simulation of the deployment-related stressors (e.g. sleep loss, harsh weather) and austere, resource-limited conditions in which military medical officers work. During the simulation, students treat ~150 simulated patients while facing continuous scenarios designed to evoke stress – including simulated enemy attacks and mass casualty events – and coping with chronic uncertainty about their next challenge [15].
Participants in the qualitative and quantitative studies (n = 23 and n = 21, respectively; demographics: Section S1) were fourth-year active-duty military medical students from the Air Force, Army and Navy. These individuals were recruited via purposive sampling: 1 week prior to Operation Bushmaster in 2022, all students attending the simulation (N = 176) received an email from the lead author that described the study and invited them to participate. Because participants were active-duty service members, they were not compensated for being part of this study, in keeping with Department of Defense policy. This study was ruled exempt by the Uniformed Services University of the Health Sciences Institutional Review Board (protocol number: 21-13063, decision date: 06/30/22).
The present study includes phenomenological qualitative research, which explores human experiences of a particular event or process [16,17]. In this case, the phenomenon of interest was Operation Bushmaster. Our approach to this research was hermeneutic [18]. That is, we focused on illuminating the underlying meaning of individuals’ lived experiences of stress and resilience during simulation. We used semi-structured interviews to delve into the ‘deeper layers’ of these experiences [19–21], and actively reflected on our own experiences of training-related stress and resilience to guide data analysis.
The quantitative pilot study followed an observational design. It focused on the correlations between performance during Operation Bushmaster, trait mindfulness and perceived stress levels prior to the simulation.
Data for the qualitative study came from semi-structured interviews that were conducted by the lead author and informed by interview guides (Section S2). Questions in these guides explored student experiences of stress and resilience during Operation Bushmaster. Participants were interviewed twice – once during and once at the end of the simulation. Interviews conducted during Operation Bushmaster took place during regularly scheduled 15-minute rest periods to maximize participants’ focus on them and to avoid disrupting the simulation. Due to this time constraint, the guide for these interviews featured just five open-ended questions. The guide for post-Operation interviews was longer – with seven open-ended questions. The average duration of all interviews was 15 minutes. Interviews were audio recorded and transcribed using an automated service.
Data for the quantitative pilot study came from a brief survey that participants completed prior to Operation Bushmaster and expert ratings of performance during the simulation.
Performance was captured via expert ratings provided by military medical professionals who come from all over the world to assist with Operation Bushmaster. These individuals use standardized forms to rate students on character, competence, leadership, context (adaptability) and communication as they rotate through various roles (e.g. Platoon Leader, Surgeon) during the simulation. We focus on two performance scores: competence and the total score computed as the sum over the rated dimensions. Extra attention is paid to competence because this rating dimension specifically captures the successful demonstration of medical knowledge and performance of role-specific medical skills. All ratings were made on a 1 (unsatisfactory) to 4 (excellent) scale.
The survey contained two measures in random order:
Trait mindfulness was measured via the Five Facet Mindfulness Questionnaire [22]. Respondents rate (on a 1 = Never or very rarely true to 5 = Very often or always true scale) how their experiences align with the ideals of core mindfulness facets: observing, describing, acting with awareness, non-judgemental stance and non-reactivity. Scores on each facet were summed to create a total trait mindfulness score. In the present study, this measure had excellent internal consistency (ωtotal = 0.97).
Perceived stress was measured via the Perceived Stress Scale [23]. Respondents rated the concordance between various statements (e.g. ‘How often have you felt nervous and stressed?’) and their experience over the past week on a five-point scale (0 = Never, 4 = Very Often). Ratings were summed to give a total score. In the present study, this measure had excellent internal consistency (ωtotal = 0.97).
In order to identify key themes in our interview data, we followed Colaizzi’s method of phenomenological data analysis, which focuses on accurately and authentically conveying the participants’ experiences [24]. Two members of our research team (the lead author and a medical student research assistant) read through each interview transcript multiple times to become familiar with the data and to fully understand participants’ perspectives. While reading, they independently coded the interview transcripts, noting significant statements within and across them. These codes were compiled into a codebook. Coders (lead author and Estefania Melo) then met and arranged codes into clusters and arranged clusters into major categories – the key themes of our study [25,26].
We used multiple strategies to increase the credibility of the study conclusions. We ensured that our analytic team included members with deep experience in qualitative research and mental health (lead author) and lived experience as a military medical student (Estefania Melo). The analytic team met regularly to discuss emerging study themes. In accordance with the hermeneutic phenomenological perspective, we recognized that the analytic team’s own thoughts, experiences, and ‘lifeworlds’ were inseparable from the analysis process [17,21,27]. The analytic team, therefore, engaged in constant self-reflection – analysing their own understandings of stress, resilience and the ways these did or did not align with participants’ lived experiences – to ensure that data were reported authentically. Our study design was carefully curated to enhance the conclusion credibility. We used prolonged engagement with participants, interviewing them twice during Operation Bushmaster to gain a robust understanding of their experiences of stress and resilience. We also engaged in member checking. Participants were emailed their interview transcripts and given the chance to add, remove or modify their content. Eight participants responded to these emails. Two requested only typographical/grammatical changes. Zero participants requested changes to transcripts’ substantiative content. Finally, to ensure that readers can evaluate the trustworthiness of our results and develop a rich understanding of the phenomena and key themes we describe, in the Results section, we provide a ‘thick description’ of participant experiences via direct quotes [16,17,25].
We used non-parametric correlations (Spearman’s Rho) to examine bivariate relations of expert-rated performance during Operation Bushmaster with perceived stress prior to the simulation and trait mindfulness. This analytic strategy can accommodate non-Gaussian data distributions and minimizes the impact of individual data points, which was desirable given our small sample size.
Participants’ self-reported stressful experiences during Operation Bushmaster could be broadly grouped into two categories: internal and external stressors. There were two commonly reported internal stressors – uncertainty and fluctuating motivation – and two commonly reported external stressors – environment and equipment-related challenges. These themes and subthemes in participant narratives are described in more detail later.
One major internal source of stress for participants was ongoing uncertainty about the challenges that would be faced at Operation Bushmaster. For example, one participant (P11) reported that the ‘biggest stress was in preparation, like just not knowing how the simulation was going to be run and what the Torbian [simulated-country] days were going to look like’. Another participant (P3) emphasized that at Operation Bushmaster ‘you don’t know what you’re getting yourself into every four hours’. The second major internal source of stress for participants was fluctuating motivation across Operation Bushmaster. For example, one participant (P4) described being stressed by the struggle to stay focused during this multi-day, fast-paced simulation: ‘I was like going strong, going strong, going strong, and then suddenly … I was kind of done’. Participant narratives, including one participant’s (P10) explanation that ‘coming out here and feeling like you’re failing after failing, kind of in a way, that can be a little bit morally degrading’, suggested that some fluctuation in motivation was related to the continuously challenging nature of Operation Bushmaster.
In addition to these internal struggles, students also faced external stressors at Operation Bushmaster, such as a harsh environment. Weather was a major environment-related stressor. Participants noted that ‘it was cold, really, really cold. And I don’t think any of us were really prepared for that and to be outside all day’ (P5) and ‘[the] real morale killer for me was just always being cold’ (P23). Participants also indicated that the rocky groundcover interfered with sleep, stating that ‘gravel was not something I was expecting to be a huge factor in my sleep. I thought the cold would be the main thing, but it was not. It was the gravel’ (P2) and that ‘sleeping out in the gravel, that was tough’ (P19). Participants may not have fully anticipated how stressful environment-related factors would be. Consistent with this notion, one individual (P18) reported that they ‘underestimated the effects of working long hours and not sleeping much and sleeping uncomfortably’. Environment-related stress seemed to interact with other stressors. As one participant (P16) explained, Operation Bushmaster was ‘physically demanding, also mentally demanding. I have a lot of stress in all kinds of elements from all difficult paths. Can’t physically sleep. Food, I barely ate all day’.
Equipment management was another frequent source of external stress at Operation Bushmaster. Some of this was due to the physical demands of the equipment. As one participant noted, ‘the bulkiness of everything definitely slows you down in your movement and hinders how expeditiously you can deal with everything … so all of that makes you feel very slow, and that is also very stressful’ (P2). This sentiment was echoed by another participant (P17), who described Operation Bushmaster as ‘really tiring, this body armor is heavy’. Difficulties with equipment management sometimes prompted social concerns. For example, ‘having a really hard time keeping up with the lifting and running around with litters … then feeling like I’m not pulling my weight because I’m having a hard time keeping up physically’ (P22).
In response to these challenges, the students described resilience as a result of four major factors: team support, mindfulness practice, positive self-talk and ability to shift perspectives (Figure 1).

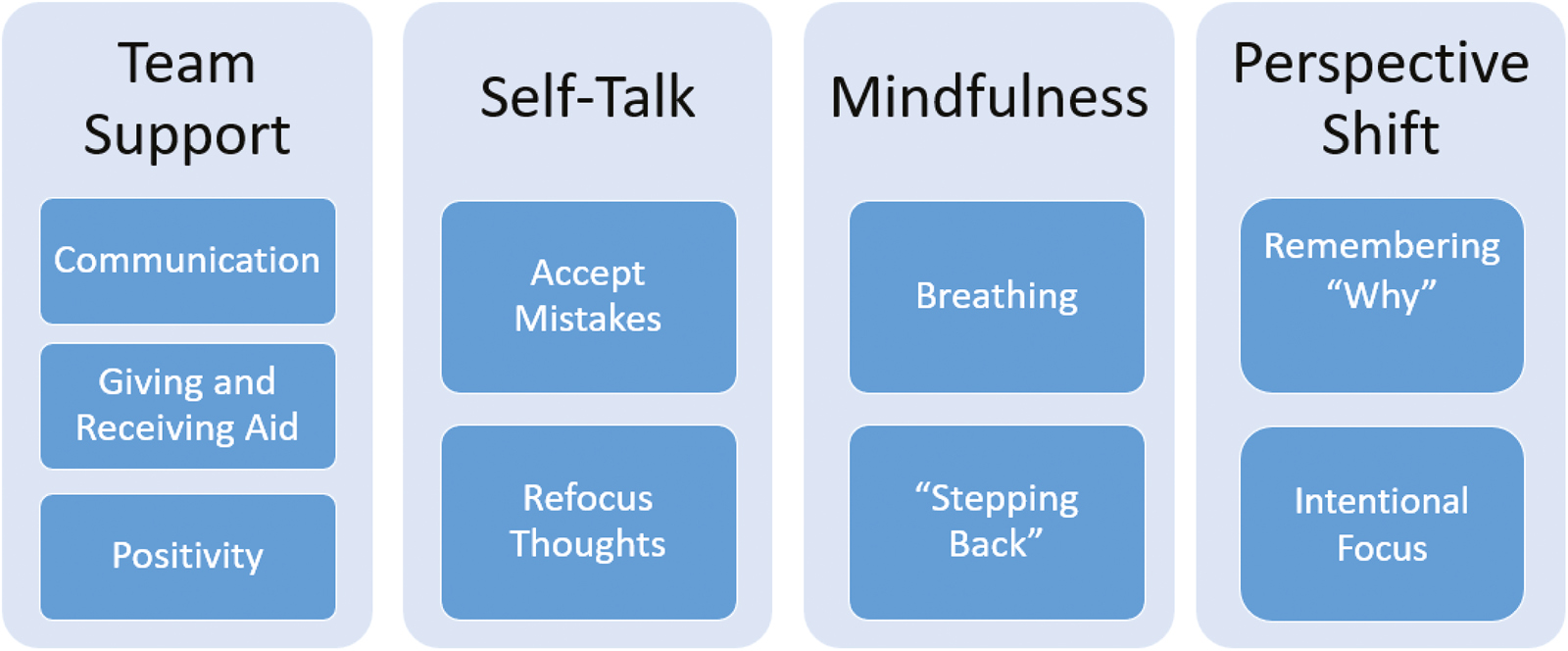
Resilience themes and subthemes that emerged from participants’ narratives about their experiences during Operation Bushmaster.
Three specific components featured prominently in participant narratives of team support:
(1) Communicating with teammates helped participants navigate the stressful aspects of Operation Bushmaster. As one participant (P20) noted, ‘having people I could talk to helped with resiliency’. Another (P11) elaborated, ‘really leaning on people and letting them know I’m tired, I’m irritated, I’m frustrated with things … just leaning on my team was very helpful’. Talking with teammates about stressors and frustrations likely buffered against stress in part because it led to a sense of connectedness through shared experience. Consistent with this notion, Participant 16 stated, ‘just talking to people … I realized that some people understood the situation, that I wasn’t alone’. Talking with teammates about one’s stressors and frustrations also fostered resilience because it afforded the opportunity to assist teammates with their own hardships. As Participant 13 noted, ‘if you’re helping others [in this manner] … it makes other stuff easy’.
(2) Giving and receiving aid to teammates was a second source of resilience, consistent with Participant 13’s statement above. For example, in response to weather-related stressors, ‘people would be like “hey man, here’s a hand warmer you weren’t even thinking of”’ (P23). Such prosocial behaviours fostered social connectedness. One participant alluded to this link, stating, ‘having my buddies around me to help … I think the resilience comes from my friends’ (P17). Another was more explicit:
We all know we can rely on each other. And even when you’re in a stressful position, like team leader or surgeon, we’re all there like helping each other…there’s still support from our classmates that helps it not feel like we’re on our own. (P5)
(3) Teammates’ positivity was a third contributor to resilience:
Relying on positive people and then trying to be positive and spread that positivity, is kind of a way to combat the suck and embrace the suck. And just every opportunity is an opportunity to learn. (P14)
Another described the role of team humour in positive thinking:
I think our platoon particularly gelled very well compared to others. So, I think that made it very easy to be resilient even in these bad situations. Even when the lights are off and we’re going to bed, everybody’s laughing and joking around. (P18)
A positive communication style also conferred resilience when it manifested as positive self-talk that helped participants accept mistakes and re-focus thoughts. One participant (P5) reported repeatedly telling themselves, ‘“it’s ok to make mistakes.” And that took the pressure off’, then elaborated that they ‘tried to fall back on a lot of my experiences knowing “Yes, I have to make a decision. If it’s a wrong one, then that’s ok”’ (P5). After making mistakes, participants engaged in future-focused positive self-talk. For example, one participant told themselves, ‘ok you still have some time left. You can still improve, you can still do this’ (P8). Other future-focused self-talk centred on the time-limited nature of Operation Bushmaster. As one participant noted, ‘the mindset is just get through this little period and deal with it and then you’ll be fine’ (P23). Another explained that, ‘you always know that, no matter how difficult it’s going to get, it’s over in a couple of days’ (P15). Self-talk was also used to plan and focus in the presence of stress. For example, Participant 6 told themselves, ‘ok, do this thing, on to the next thing. And thinking about it that way [rather] than being [hyper-]aware of all of the chaos. I need to be aware of it, but not overwhelmed by it’. Finally, self-talk was used for emotion regulation, via self-communications like, ‘“I need to take a breath and know that normally this wouldn’t bother you”’ (P4).
Many participants reported managing stress with intentional or mindful (‘tactical’) breathing – which was taught (alongside other mindfulness skills) in a brief session prior to Operation Bushmaster. This technique allowed them to slow down and take space during stressful situations. As one participant explained:
Breathing with the patient as you’re BVMing [bag-valve-masking], it taught us about tactical breathing. So that was useful as far as, not only falling asleep, but as well as before getting out of the LMTV [Light Medium Tactical Vehicle] or FLA [Field Litter Ambulance], just taking a moment to yourself. (P14)
Breathing was also used to facilitate paying attention to the present moment on purpose:
I did some of the mindfulness exercises … I did breathing and I kind of just stopped a little bit and tried to like look around at what’s happening, like try to see the situation from outside as much I could, and that was helpful in roles where I was stressed out ... I would try to just like center myself a little bit by just focusing on my breathing. (P8)
Participant 19 also used breathing techniques to focus, step back and slow down:
If I started to feel like I was running around a little crazy, I would take a step back, assess the whole situation, and try to focus in on what I could do right now that would make the team better … step back, take a breath.
Some participants explicitly attributed strong performance and leadership to mindful breathing. One stated that,
I always need to take a step back and breathe a little bit. I talk really quickly, and so on a mental process, I’m spitting out the information. But being able to step back, look at who is working with me, and say, ‘Ok, we are going to do this in a calm and collected manner that’s not like rapid fire,’ it just helps to communicate the plan going forward. (P3)
Another echoed:
I felt like most of the time I was like ‘take a deep breath’ … sometimes when I briefed, I would start speaking fast and then I would find myself like ‘Ok, I’ve got to come back and find my breath’. (P12)
Participants also shifted perspectives as a way to overcome the challenges of Operation Bushmaster. Several participants did this by recalling the meaning behind their experience at the simulation. For example, Participant 4 explained how:
In the moment it sucks, but if you step back and evaluate the reason that you’re there and try to find the positives in whatever situation, focus on those, and then just make sure you have your mind on the ultimate goal, which is to get better and learn.
Participant 7 connected this learning to the military’s medical mission:
I knew that I have to be ready when I’m called upon to take care of sailors, airmen, marines, soldiers, that I am ready as I can be…I need to get this under my belt…If I have to do this in three years, in four years, in five years, I want to be ready.
Another echoed Participant 4’s focus on an ultimate goal, describing how they ‘just keep pushing forward, I just think about the future. I wanted to finish Bushmaster and I want to become a doctor’ (P16).
Flexible deployment of attention, a key part of perspective shifting, also played a prominent role in participants’ narratives. Some oriented attention towards controllable stressors over less controllable ones. As Participant 4 described:
I tried to keep track of what I needed … I made sure that I had water, I made sure that I ate, I made sure that I stayed warm … so I was really, really conscious about that and keeping track of my equipment, that really helped me then to be focused on what needed to happen.
Others echoed this theme of intentionally focusing on what was controllable, stating that:
I was able to change my mindset and be like, ‘Ok, how can I help our team to get through this iteration and be more effective than they were last iteration?’ And so I think instead of just focusing on how worried I was and trying to see how I could help out in other ways, helped me to focus less on my stress. (P5)
Descriptive statistics were as follows: Competence M = 3.13 (standard deviation [SD] = 0.33). Total Performance M = 15.77 (SD = 1.00). Trait mindfulness M = 141.48 (SD = 20.51). Perceived stress M = 11.43 (SD = 6.52). The correlations of stress with total performance (rho = −0.35, p = .116) and competence (rho = −0.24, p = .301) were not statistically significant. In contrast, the correlation between trait mindfulness and total performance ratings was statistically significant, rho = 0.45, p = .042. There was also a trend-level correlation between trait mindfulness and competence ratings, rho = 0.41, p = .065. These relations between performance and mindfulness are visualized in Figure 2.
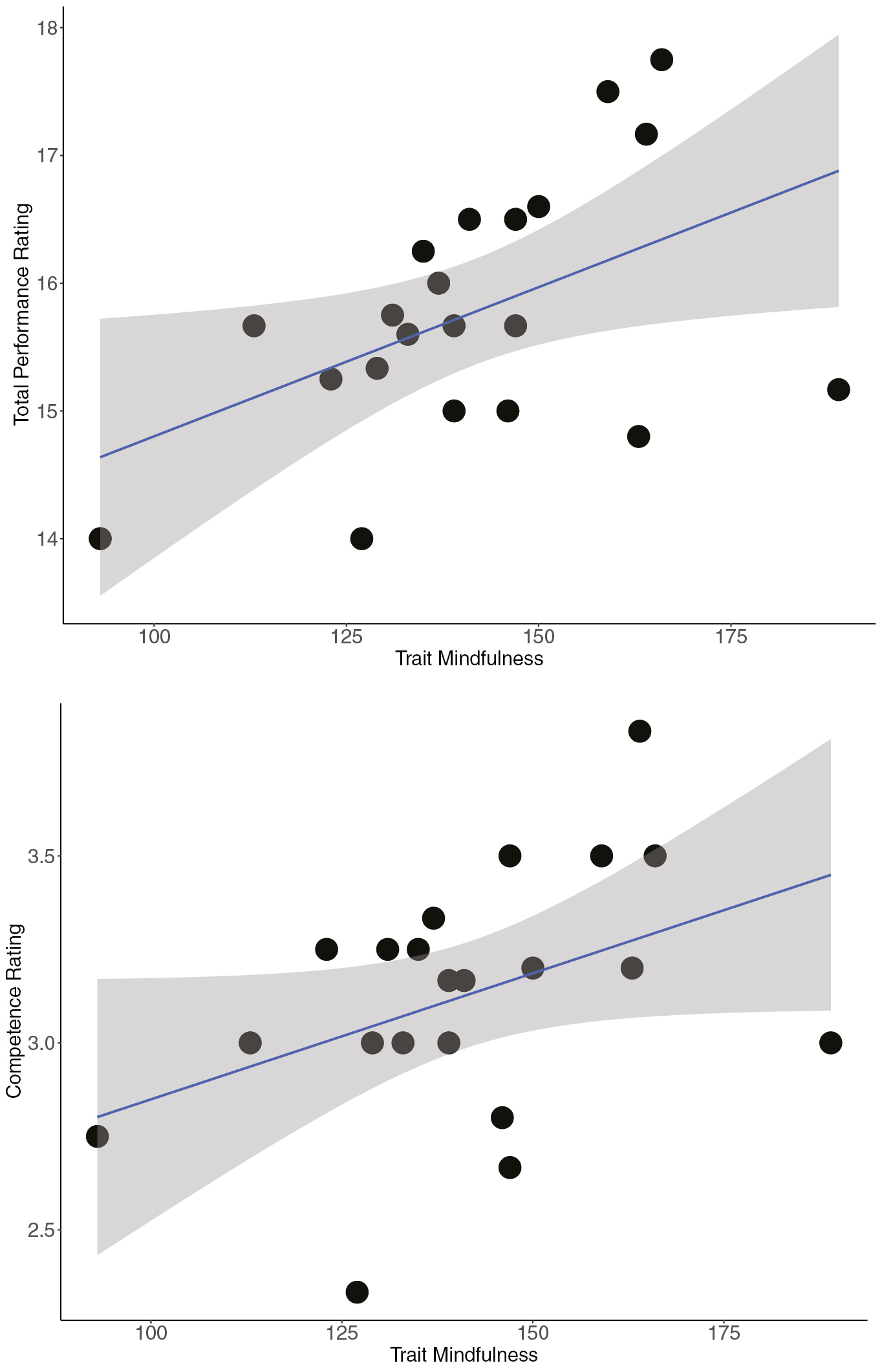
Relation of trait mindfulness with total performance ratings (top) and competence ratings (bottom). Clouds are 95% confidence intervals (CIs). FFMQ = Five Facet Mindfulness Questionnaire.
The present study characterized lived experiences of stress and resilience via qualitative interviews conducted during Operation Bushmaster – a well-established annual simulation where students make medical decisions and perform medical procedures as part of a high-fidelity simulated deployment. The narratives of fourth-year military medical students revealed common external (equipment and environment-related factors) and internal (uncertainty and fluctuating motivation) stressors. Narratives also pointed towards major sources of resilience against stressors, including team support, mindfulness, positive self-talk and perspective shifting. A small quantitative study built on these narratives by suggesting that trait mindfulness (but not stress levels prior to the simulation) was associated with expert-rated performance at Operation Bushmaster. The emergent themes of our qualitative research are critical leverage points for educators seeking to optimize management of stress levels during their own simulation; these themes also have rich connections to existing literature on stress and resilience.
The strong connection between the present study and past literature on mindfulness is particularly notable. Previous research in military and non-military settings demonstrates that mindfulness causes stress reduction [28,29]. In medical students specifically, contemplative practice interventions that increase mindfulness are associated with improved psychological well-being [8] and trait mindfulness correlates with improved performance (fewer medical errors) during high-fidelity simulations of paediatric medical emergencies [9]. These findings are echoed by studies of professional medical teams, who perform better when treating simulated cardiac arrest after a mindfulness mediation intervention [30]. The present study builds on this past work by showing that participants in a well-established high-fidelity military medical simulation perceive a link between their mindfulness skill use and their ability to effectively lead and care for others. In a small quantitative pilot study, we found support for this perception in the form of a moderate positive correlation between trait mindfulness and expert ratings of the medical knowledge/skill that students demonstrate during Operation Bushmaster (Figure 2). Taken together, our qualitative and quantitative data provide a compelling basis for future experimental studies testing whether mindfulness causally affects medical students’ skill/leadership under stress, or whether the reverse is true. They also suggest that mindfulness training could be a valuable tool for modulating stress such that high-fidelity simulations are more likely to yield the desired medical learning and gains in coping skills [5].
Our results also interface closely with previous literature examining how team dynamics modulate performance under stress. This literature highlights social cohesion – defined as shared social identity and orientation towards maintaining relationships among team members – as a key resilience factor [31]. Socially cohesive teams are thought to be more resilient because they offer members social support and healthy distraction [32]. Among medical teams, cohesion appears to improve care for others in austere, stressful environments [33]. Communicating with realistic positivity and a culture of mutual aid are also associated with resilience [12]. In accordance with this research, our participant narratives link resilience to healthy distraction (e.g. laughing and joking with teammates before going to sleep [P18]), social support (e.g. sharing frustrations with and leaning on teammates [P11]), mutual aid (e.g. sharing of hand warmers [P23]), and realistic positivity (see quotes from P14). Future research should build upon this study by examining which of these factors is most strongly related to students’ medical leadership and overall medical team performance in austere, stressful environments, like that in Operation Bushmaster. Such research should also investigate how factors that modulate social cohesion, such as prior experience with teams or classic group identity manipulations [34], impact student experiences during and key outcomes of high-fidelity simulation training.
When considering the implications of our study, readers should be aware of several limitations. Our qualitative research focused on one particular simulation that mimics deployment (Operation Bushmaster) in a military medical school. Results – especially those concerning external sources of stress – may not generalize fully to other simulations, particularly those implemented in civilian settings. A second limitation is that we did not follow up with participants to examine how this experience influenced their post-Bushmaster experiences of stress and resilience. However, our prior research suggests that Operation Bushmaster prepares students to successfully navigate stressful situations (e.g. those involving suicidality) they encounter during their first deployment [35]. From a hermeneutic perspective, we also recognize that the lived experiences of the research team can influence the analysis of qualitative data, though we took steps to mitigate this (see Methods). Our quantitative study also has limitations. The correlation we found between trait mindfulness and expert-rated performance at Operation Bushmaster may or may not reflect a causal relation between these variables. The lack of correlation between anticipatory stress and expert-rated performance is likely due to our small sample size and limited statistical power, as many previous studies have found performance–stress relations. Moreover, the relation between stress and performance is likely to be stronger when stress is measured contemporaneously, rather than prior to the performance period.
The present study identified major sources of stress and resilience experienced by advanced military medical students attending Operation Bushmaster, an annual military medical high-fidelity simulation. These stress and resilience factors are critical leverage points for educators seeking to optimize learning and skill development during Operation Bushmaster. Many, if not all, resilience factors we identified are also likely relevant to civilian medical education and associated simulations. Future research should continue to examine how the balance of stress and resilience factors during these types of simulation impacts medical students’ immediate learning (e.g. regarding medical decision-making, skill performance and leadership) and longer-term ability to successfully navigate the stressors of the medical profession.
The authors acknowledge Estefania Melo for her contributions to data analysis. The authors also wish to thank the student volunteers for participating in this study and Dr. Sophia Vinogradov for her helpful comments on this manuscript. The opinions and assertions expressed herein are those of the authors and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences or the Department of Defense.
RC and MB conceptualized and designed the study. RC collected study data. RC and MB analyzed and interpreted the data, drafted the manuscript, and critically revised the manuscript.
None declared.
This study was ruled exempt by the Uniformed Services University of the Health Sciences Institutional Review Board (protocol number: 21-13063, decision date: 06/30/22).
RC and MB report no conflicts of interest.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
 Stress and resilience among military medical students completing a high-fidelity military medical simulation
Stress and resilience among military medical students completing a high-fidelity military medical simulation
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets