
Patient profiles have changed from shifting demographics, globalization and immigration. Such changes highlight the need to educate and train healthcare trainees and healthcare providers (HCPs) on the provision of person-centred care through an equity, diversity and inclusion (EDI) approach. Simulation pedagogy has the potential to be a useful and impactful teaching and learning approach for EDI. The purpose of this review was to explore and summarize the current literature on the level of integration and state of EDI in clinical simulation within healthcare education, curricula and training.
An integrative literature review was conducted using Whittemore and Knafl’s (2005) method. Studies that met the selection criteria were assessed using the Johns Hopkins Nursing Evidence-Based Practice Model.
A total of 64 studies were included in the review. Five themes emerged from EDI incorporation in clinical simulation education and training for HCPs and healthcare trainees: (1) increase in self-awareness; (2) enhanced communication; (3) enhanced insight and knowledge; (4) strengthened EDI-related self-efficacy; and (5) increase in EDI-related competence and skills.
Clinical simulation provides opportunities for EDI integration in healthcare education. Several implications were identified: (1) employing a more systematic process for EDI integration in healthcare education and programs; (2) developing a digital repository of EDI-focused clinical scenarios; (3) co-creating EDI-focused clinical simulations with persons of diverse background; (4) the importance of maintaining a safe learning environment for all involved persons – learners, staff, faculty and standardized/simulated patients in the EDI simulations; and (5) the need for more robust and rigorous research to advance the science of clinical simulation.
What this study adds
In Canada, persons of diverse racial and ethnic background are projected to comprise a third (31–36%) of the population by 2036 [1]. Similarly, in the United States, it is projected that by 2060, 32% of the population will be non-white (equating to one in three persons) [2]. Empirical evidence suggests that health disparities exist for persons of diverse ethnic, racial and gender and sexual backgrounds. Such disparities are rooted in colonization, implicit and explicit bias as well as individual, institutional and structural racism [3]. Such biases and racism result in poor health outcomes, quality of care and access to care, compromises patient’s well-being as well as increases medical errors, safety and adverse events [4–9].
A strategy to mitigate or minimize biases, racism and inequities experienced by patients is through diversity education [3]. Diversity education requires a culture shift and intentional efforts to re-structure healthcare education, training and curricula that pays explicit attention to cultural safety and humility; equity, diversity and inclusion (EDI); and addresses biases as well as individual, institutional and structural racism [10–13]. Such EDI education builds a workforce that is more responsive to diverse patient populations as the healthcare trainees and healthcare providers (HCPs) possess the critical skills and awareness of their position of power and privilege and the impact this has on patient–provider interactions and care [14].
Interactive and experimental methodologies, such as clinical simulation, may be an avenue to provide EDI education. The science of clinical simulation within healthcare education continues to evolve and expand as a teaching and learning approach for health science trainees and HCPs [12]. Empirical evidence suggests that clinical simulation holds great promise in improving the knowledge and skills of healthcare trainees and HCPs and contributes to improving patient safety and care [15–17]. This is because clinical simulation facilitates the transfer and application of learning to practice through realistic clinical scenarios and provides a safe environment for healthcare trainees and HCPs to practice skills (e.g. clinical, communication and interprofessional) on complex and sensitive topics and situations such as those that may arise regarding EDI [12,18,19]. For example, clinical simulation was found to be effective in improving nursing and medical students’ ability to conduct culturally focused assessments, and palliative care, use more inclusive language, and be more culturally aware. This was further coupled with noted improvement in nursing and medical students’ confidence and competence in treating patients who are two-spirit, lesbian, gay, bisexual, transgender, queer and/or questioning, intersex, asexual (2SLGBTQIA+) [20–23].
Although clinical simulation has the potential to be a useful and impactful teaching and learning approach for EDI, limited empirical evidence exists on the extent to which EDI is integrated into clinical simulation within healthcare education curricula and/or programs [12]. Such an understanding is imperative with the commitment of EDI across healthcare systems, academic institutions and learning health systems. This is further coupled with the impact on addressing biases, racism, health inequities and disparities; all of which if addressed may improve patient health outcomes, and delivering inclusive, diverse and culturally safe care [24–27]. The aim of this review was to explore and summarize the current literature on the level of integration and state of EDI in clinical simulation within healthcare education, curricula and training.
We followed Whittemore and Knafl’s [28] integrative literature review method. This method allows for a comprehensive understanding of the phenomenon under investigation by including diverse research methodologies [28]. The method consists of five steps: (1) identifying the problem of interest; (2) conducting a comprehensive literature search; (3) evaluating the quality of the studies; (4) conducting a data analysis; and (5) drawing conclusions and presenting findings.
The literature searches were conducted by a Health Sciences Librarian on 22 July 2021. The databases used to retrieve relevant publications were Ovid MEDLINE (Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid MEDLINE® Daily and Ovid MEDLINE® 1946 to Present), Ovid Embase + Embase Classic (1947 to 21 July 2021), EBSCO CINAHL Plus with Full Text (1981 to present), OVID APA PsycInfo (1806 to Present), ProQuest ERIC, Wiley Cochrane Central and Web of Science Core Collection. Details of the keywords and Boolean operators are presented in Appendix A. A combination of database-specific subject headings and text words was used to search for the concepts of simulation and cultural humility as well as relevant synonyms. No limits or filters were applied. A draft of the Ovid Medline search was peer-reviewed prior to search translation by a second health sciences librarian using the PRESS guidelines [29]. Search results were deduplicated in EndNote using the optimized method by Bramer et al. [30], then uploaded to DistillerSR where remaining duplicates were identified.
Articles were included in the review if the following selection criteria were met: (a) the sample represented healthcare trainees and/or HCPs (e.g. nursing, medicine, physical therapy, occupational therapy, social work, pharmacy, etc.); (b) all methods of simulation (high fidelity, low fidelity, virtual [e.g. virtual reality, serious gaming, etc.], standardized/simulated patients, etc.); (c) focus on EDI within clinical simulation as part of healthcare curricula, education or training; (d) academic and/or community institutions and health science centres; and (e) papers written in English. The article review process was conducted by three authors (SI, BS and NT).
The quality of the studies that met the selection criteria was assessed using the Johns Hopkins Nursing Evidence-Based Practice Model [31]. The studies were assessed using the research evidence appraisal tool. The level of evidence was determined by the study design and the quality of each study was scored as yes, no or not applicable, and rated as ‘high quality’, ‘good quality’ or ‘low quality/major flaws’. Two authors independently performed the quality assessment and convened to reach the final consensus.
Data were extracted on the study characteristics, mode of simulation, study findings and recommendations. The following information on the study characteristics was extracted: (a) author’s last name(s) and publication date; (b) country in which the study was conducted; (c) research design; (d) setting; (e) discipline; (f) type of simulation; (g) other/additional educational resources employed; (h) target patient population; (i) outcomes of interest; and (j) study findings.
Data analysis consisted of data reduction, data display, data comparison, and drawing conclusions and verification [28]. Specific to data reduction , an initial subgroup classification process was developed based on the study characteristics (e.g. sector, type of technology and participant characteristics) and findings. Descriptive statistics of the study characteristics were also analysed using Statistical Package for Social Sciences Version 29.0 (SPSS 29.0) [32, 33]. Specific to data display , the extracted data were converted into a summary chart to enhance the visualization of patterns within and across the data sources [28]. For data comparison, data examination was an iterative process where key concepts were recorded and tabulated for frequency, informing the development of the themes. For drawing conclusions and verification, the first author reviewed and cross-checked the extracted data. The first and second authors conducted the data analysis. The findings were reviewed by all authors for analytical agreement.
The literature search yielded 8791 titles and abstracts. Of these, 2397 were excluded because they were duplicates. Of the remaining 6394 articles, 30 were excluded because they were abstracts, books or book chapters. Initial title and abstract screening were conducted on 6364 articles. Of these, 6296 articles were excluded for not meeting the selection criteria. A total of 68 articles were reviewed in full text with three excluded due to the low-quality evidence score and one for not meeting the selection criteria. A total of 64 studies were included in this review (Figure 1). Although the studies were lower in the hierarchy of evidence, the majority of the studies were rated as good quality (n = 63, 98%), and one was high quality (1.5%) [33].

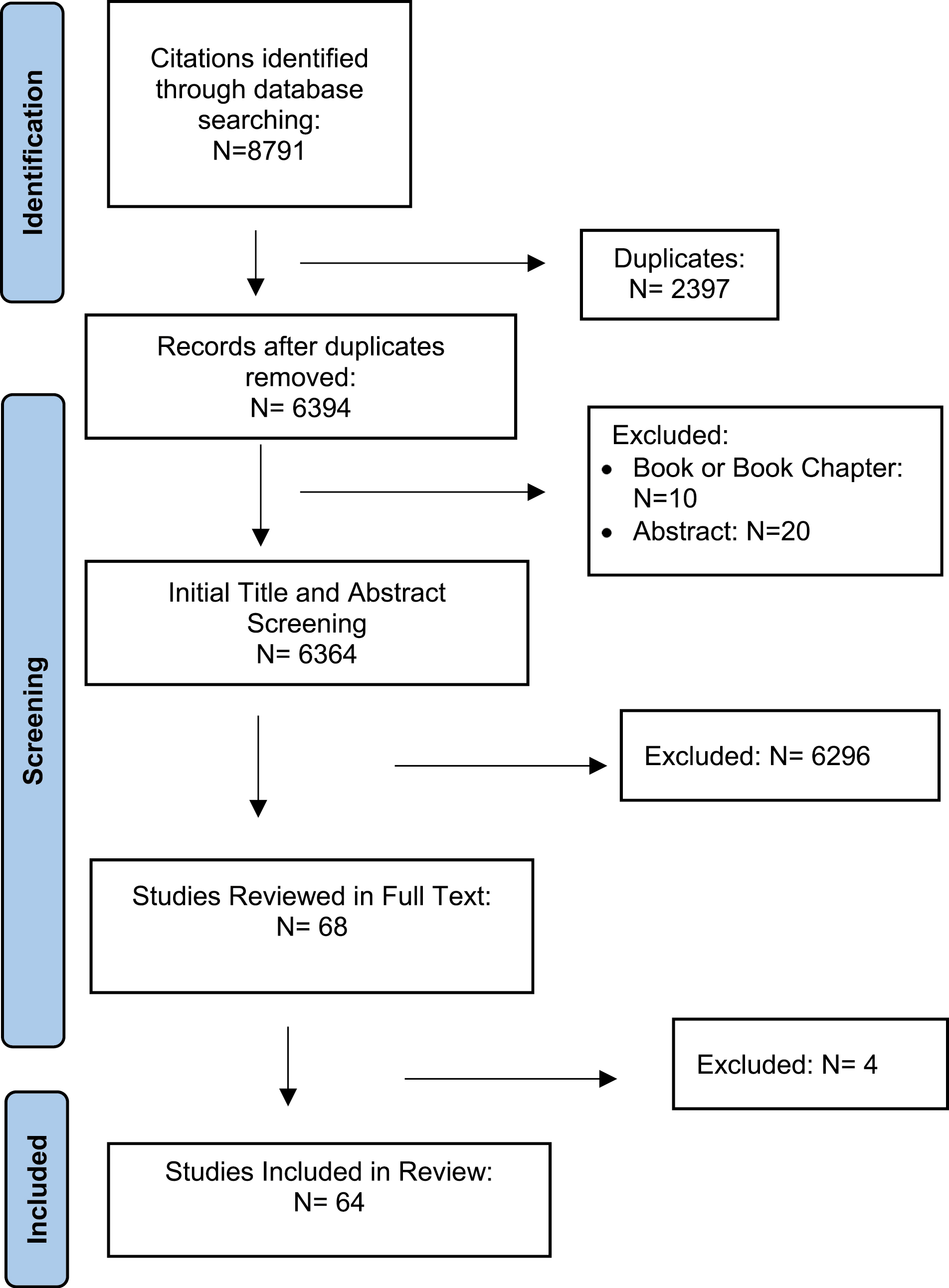
PRISMA flow diagram.
A total of 64 studies published between 2002 and 2021 were included in this review. The majority of the studies were conducted in the United States (n = 47, 73.4%). Most of the study designs were quantitative (e.g. cross-sectional, pre-post, survey design and descriptive) (n = 41, 64.1%) and conducted in an academic setting (e.g. college or university) (n = 54, 84.3%). The discipline of the studies varied with most being nursing (n = 30, 46.9%), medicine (n = 9, 14.1%), pharmacy (n = 4, 6.3%), nurse practitioners (n = 3, 4.7%), social work (n = 2, 3.1%), dentistry (n = 2, 3.1%), physical therapy (n = 1, 1.6%), midwifery (n = 1, 1.6%), as well as general HCPs and healthcare trainees (n = 12, 18.7%) (Table 1).

| N | % | |
|---|---|---|
| Country of publication | ||
| United States | 47 | 73.4 |
| Canada | 4 | 6.2 |
| Australia | 5 | 7.8 |
| Finland | 1 | 1.6 |
| Indonesia | 1 | 1.6 |
| South Korea | 1 | 1.6 |
| Sweden | 1 | 1.6 |
| Switzerland | 1 | 1.6 |
| Thailand | 1 | 1.6 |
| Australia and Hong Kong | 1 | 1.6 |
| United States and Norway | 1 | 1.6 |
| Study design | ||
| Quantitative | 41 | 64.1 |
| Qualitative | 8 | 12.5 |
| Review | 6 | 9.4 |
| Quasi-experimental | 5 | 7.8 |
| Mixed methods | 3 | 4.6 |
| Randomized clinical trial | 1 | 1.6 |
| Setting | ||
| Academic (i.e. college or university) | 54 | 84.3 |
| Acute care sector | 3 | 4.7 |
| Community care sector | 1 | 1.6 |
| Combined settings (i.e. acute care, home care and academia) | 6 | 9.4 |
The type of simulation employed in the studies varied. Most studies employed standardized/simulated patients (n = 39, 60.9%) and the majority (n = 41, 64.1%) reported using simulation in conjunction with other educational activities (Table 2). The educational activities varied and included: modules, role play, debates, case vignettes, video presentations, lectures, assigned readings, group discussions (in-person and online) and a reflective journal.
| N | % | |
|---|---|---|
| Type of simulation | ||
| Standardized/simulated patients (SP) | 39 | 60.9 |
| Virtual reality | 13 | 20.3 |
| Hybrid | 5 | 7.8 |
| eSimulation module | 1 | 1.6 |
| Low fidelity using role play | 1 | 1.6 |
| Simulated care vignettes | 1 | 1.6 |
| Video simulated scenarios | 2 | 3.1 |
| Simulation game | 1 | 1.6 |
| Combination of methods (i.e. virtual reality and SP) | 1 | 1.6 |
| EDI concepts in simulation learning objectives | ||
| Cultural competence | 43 | 67.2 |
| Cultural awareness | 7 | 10.9 |
| Knowledge, skills & attitudes towards diverse cultures & populations | 4 | 6.3 |
| Cultural communication | 2 | 3.1 |
| Cultural empathy | 2 | 3.1 |
| Cultural empathy & sensitivity | 2 | 3.1 |
| Cultural humility & interviewing skills | 1 | 1.6 |
| Culturally focused interviewing & physical examination skills | 1 | 1.6 |
| Awareness of personal biases & interviewing skills | 1 | 1.6 |
| Cultural sensitivity | 1 | 1.6 |
The target patient population for the simulation scenarios in the studies varied and included persons of Chinese, Arab, African, Amish, Somalian, Indigenous, Latino and Italian backgrounds as well as non-conforming and 2SLGBTQIA+. Several studies also focused on persons whose social determinants of health were compromised (e.g. food insecurity, poverty, living in rural and remote areas), were pregnant, non-English speaking and palliative.
The studies addressed various EDI concepts as learning objectives and aims of the simulations with cultural competence being the most (n = 43, 67.2%) commonly reported (Table 2). A total of five themes emerged from the incorporation of EDI in clinical simulation education and training for HCPs and healthcare trainees. The themes were: (1) increase in self-awareness; (2) enhanced communication; (3) enhanced insight and knowledge; (4) strengthened EDI-related self-efficacy; and (5) increase in EDI-related competence and skills.
The first theme that emerged as an outcome of the in-person and virtual reality simulations was the noted increase in HCPs’ and healthcare trainees’ self-awareness of their own biases, beliefs, values, attitudes and assumptions. The HCPs and healthcare trainees noted that their biases, assumptions and values influenced their interaction and approach with persons of diverse cultural, ethnic, racial and gender backgrounds during the clinical simulations. The increase in self-awareness among HCPs and healthcare trainees was noted in several studies. For example, Tiffany and Hoglund [34] found that the graduate nurse educator students who participated in the virtual reality simulation became aware of their biases as well as the influence those biases had on their behaviour and interaction with the avatars. Similarly, in Kourgiantakis et al.’s 2020 study [35] that explored how social work students conceptualize culture and diversity after interviewing a standardized/simulated patient found that some students became aware of their biases (e.g. gender) and assumptions. The students also reflected on how their biases and assumptions were projected in the interviews, approach and topics discussed with the standardized/simulated patient [35]. Interestingly, in Weideman et al.’s study that explored the impact of virtual reality simulation on nursing students’ cultural competence, it was noted that Amish and African American community participants (who collaborated in the simulation design and simulation) were occasionally offended by the way in which nursing students framed their questions and the assumptions made about their respective cultures [36]. Following participation in the simulation, some of the nursing students were able to identify and recognize the importance of providing care that was non-judgemental, assumption-free and unbiased [36].
The second theme that emerged as an outcome from the simulations pertained to the enhanced communication among the learners, which supported the provision of culturally competent care and the ability to establish a safe and respectful atmosphere. For example, in Hickerson et al.’s [22] study, nursing students who participated in the simulation program reported an improved ability to use inclusive language with LGBT patients and confidence in establishing a safe and respectful environment for this patient population. Similarly, in Maar et al.’s study on the co-creation of simulated cultural communication scenarios for Indigenous persons, participation in the simulation was found to support medical students and tutors in being able to foster authentic and safe environments by using anti-oppressive language and dialogue [37]. The improvement in communication skills extended beyond the standardized/simulated patients and towards members of the interdisciplinary team. For example, when 73 nursing students participated in a simulation where they played the role of members of the interdisciplinary team (e.g. pharmacists, physicians, physical therapists), 69% indicated an improvement in their communication skills, which has implications for the provision of person-centred care [36].
The third theme that emerged was the noted increase in HCPs’ and healthcare trainees’ insight and knowledge about diverse cultures, persons, populations and challenges experienced (e.g. navigating the healthcare system, language, financial, housing and access). For example, there was a statistically significant increase in knowledge about Arab American Muslims among medical students who participated in an online interactive simulation [33]. In a poverty simulation that was promoting culturally competent care in community health nursing, the survey findings revealed a significant increase in nursing students’ general understanding of persons living in poverty, the barriers experienced in accessing healthcare, financial pressures and emotional stresses [39]. Similarly, there was a statistically significant increase (p = 0.001) in culture-related knowledge among nurse practitioner students who participated in a 20-minute health interview with an African American standardized/simulated patient. The nurse practitioner students appreciated having an opportunity to discuss and learn about the African American patient’s culture and better understand how it affects their overall health and care [40]. Lampiris et al. also found an increase in knowledge among dental students who participated in a poverty-focused simulation. The increase in knowledge pertained to the challenges experienced by low-income families, such as financial pressures, emotional stressors as well as access to community resources [41].
The fourth theme that emerged was the strengthened EDI-related self-efficacy among the learners when participating in simulations for diverse patient populations and situations. The strengthened self-efficacy pertained to performing cognitive (knowledge), affective (attitudes, beliefs and values) and practical (interview) skills [36,39,42,43]. For example, there was a statistically significant increase in overall and subscale post trans-cultural self-efficacy scores (p < 0.001) for nursing students who participated in a virtual reality simulation on African American and Amish patients. More specifically, improvements were noted in nursing students’ knowledge of cultural factors influencing care, interviewing patients from diverse backgrounds, and cultural awareness and advocacy [36]. Similarly, in a transgender-simulation patient simulation intervention, there was a significant improvement in nursing students’ self-efficacy in their skills, attitudes and knowledge in providing culturally tailored and congruent care to this patient population [44].
The fifth theme that emerged was the increase in EDI-related competence and skills. The skills encompassed communication, teamwork, collaboration, empathy, assessment and physical examinations among the learners who participated in the simulations. For example, third-year pharmacy students who participated in simulated case vignettes reported improvement in their soft skills, specifically empathy [45]. Similarly, in the poverty simulation, nursing students’ empathy greatly improved towards persons of low-income households, their attitudes towards poverty and those experiencing it [39]. Similarly, midwifery students had a significant increase in empathy following the participation in a cultural empathy workshop with a simulation component on Indigenous women and women from culturally and linguistically diverse backgrounds [46].
There has been an increased focus on the integration of EDI in healthcare and medical education with the intent of acknowledging and addressing biases, racism, as well as health disparities and inequities experienced by persons of diverse backgrounds and, in turn, improve their health, quality of care and outcomes. Simulation pedagogy has rapidly evolved in health education and training because of the ability to effectively replicate, through an immersive and interactive manner, real-life clinical scenarios in a safe, controlled and non-threatening learning environment [47,48].
In this review, the use of clinical simulation (e.g. low fidelity, high fidelity, virtual reality, hybrid and standardized/simulated patients) was found to enhance HCPs’ and healthcare trainees’ self-awareness, communication, insight and knowledge, EDI-related self-efficacy and EDI-related competence and skills. The findings from this review are consistent with that of the literature. For example, in Chae’s systematic review, it was found that virtual reality simulation was effective in enhancing cultural competence among pre-licensure and licensed HCPs [49]. Four themes (cultural sensitivity and competence; insight and understanding; communication; confidence and comfort) emerged in Foronda et al.’s integrative literature review on cultural competency and humility in simulation-based education [50]. Similarly, in San’s review of the literature, simulation was found to enhance culturally competent nursing care [51].
With research focusing on cultural-related concepts (e.g. competence and humility), this review extends beyond culture and cultural competence and contributes to the limited body of literature on EDI and clinical simulation for both healthcare trainees and HCPs. The EDI focus in simulation is integral as it enables meaningful teaching and learning, which has the potential to build a healthcare workforce that values diverse patient populations and is more responsive to the needs, beliefs and preferences of diverse and underrepresented persons coupled with dismantling covert and over biases and assumptions [12,52].
Although clinical simulation, as a pedagogy and platform, may be a promising and innovative teaching method within healthcare education to prepare and support HCPs and healthcare trainees in developing their EDI-related cognitive, affective and practical skills [53], there are two key considerations. The first consideration is that while clinical simulation reduces the harm to actual patients, the potential harm is shifted to the standardized/simulated patients [53]. The standardized/simulated patients who are recruited for their lived experiences or personal characteristics may feel the negative effects of misrepresentation, stereotyping, microaggressions and/or tokenism [53], further perpetuating biases, racism and inequities. This highlights the ethical obligation that educators have to ensure the psychological safety of the standardized/simulated patients and maintain a safe learning environment (characterized by integrity, trust, transparency and support) for all persons involved (e.g. learners, standardized/simulated patients, educators and staff) [53]. The second consideration pertains to terminology. Appreciating the recent and important discourse around EDI education in healthcare and medical programs and curricula, moving towards more inclusive language, such as cultural humility, is critical. Cultural humility is based on Leininger’s Cultural Care Theory and posits three principles that centre around life-long learning and critical reflection, awareness of power imbalance between providers and patients and institutional accountability to learners, staff, faculty, patients and communities [54]. The use of language rather than more limited ones such as cultural awareness and competence is recommended to be considered by educators.
The findings from this study have several implications. First, there is a need for more systematic processes for integrating EDI in healthcare curricula and/or programs. Interestingly, in most of the studies (63.1%) included in the review, clinical simulation was reported to be used in conjunction with other educational activities. This finding aligns with Weller et al.’s recommendation that simulation should be integrated into healthcare curricula and training and not be used as a stand-alone educational intervention [55]. In other words, EDI should be integrated into healthcare programs, with clinical simulation being one educational tool and approach that can be employed.
Second, there is a need to develop a digital repository of EDI-focused clinical scenarios that can be housed, shared and accessed by faculty, clinicians and educators across academic institutions and academic health systems [56]. The development of simulation scenarios can be quite time-consuming and is often not accounted for in faculty workload [56]. Educators and clinicians are spending considerable time and resources developing similar EDI-focused scenarios (e.g. poverty, caring for non-binary persons). As such, having a digital repository of scenarios, procedures and resources would enhance the simulation experience for all involved as well as advance the methodology, pedagogy and science of simulation [57–59].
Third, there is a need to co-create EDI-focused clinical simulations and scenarios with persons with lived experience and embodied knowledge, who represent the communities highlighted within the simulation curriculum. This co-creation is imperative for a realistic, non-tokenistic and authentic portrayal of persons and to facilitate an approach to teaching EDI from the persons’ lived experience rather than that of the educator or clinician [37,60]. Fourth, the importance of educators maintaining a safe learning environment for all persons involved in the simulation – learners, staff, faculty and standardized/simulated patients. Ethical frameworks and strategies to balance the risks and benefits of EDI in simulation and collaborating with standardized/simulated patients have been highlighted in the literature (e.g. [53]).
Finally, from a methodological perspective, there is a need for more robust and rigorous research as the studies varied in quality, rigour and design. For example, in this review, there was only one RCT and most of the studies were non-experimental and descriptive. There is also a need for more information on intervention fidelity and whether the delivery of the simulation-based initiatives or interventions is being implemented as planned and intended. This is important because intervention fidelity affects the statistical conclusion as well as external and internal validity. Such affects may result in a Type III error (which refers to failure of implementing the simulation intervention as planned), variability in outcome achievement, inflation of error variance in posttest outcomes [61,62]. Intervention fidelity may also decrease the statistical power in detecting effects, and the correct conclusions on the effectiveness of the simulation-based intervention [61,62].
The study has some noted limitations. First, the papers included in this review were limited to the English language. Second, although a comprehensive search strategy was employed, due to the broad and various terms that are used interchangeably on this topic, some articles may have been missed. Third, the authors did not look at who (e.g. faculty, persons from diverse backgrounds, etc.) developed the simulation scenarios as part of the data extraction process. Finally, the preponderance of Western authors in this literature review does introduce biases, including but not limited to publication bias.
With globalization and shifting demographics around the world, patient profiles have changed. Patients of diverse backgrounds have been found to experience healthcare-related challenges and inequities. The incorporation of EDI within healthcare trainees’ and HCPs’ education and training is a strategy to address this challenge and build a healthcare workforce that values and effectively cares for diverse patient populations [12,50,52]. The science of clinical simulation within healthcare education continues to evolve and expand as a teaching and learning modality for health science trainees and HCPs [12]. However, there is limited knowledge of the extent to which EDI is being integrated in clinical simulation [12]. The purpose of this review was to explore and summarize the current literature on the level of integration and state of EDI in clinical simulation within healthcare education, curricula and training. A total of 64 studies were included in this review. The use of clinical simulation was found to enhance HCPs’ and healthcare trainees’ self-awareness, communication, insight and knowledge, EDI-related self-efficacy and EDI-related competence and skills. Several implications were identified from this review: (1) the need for a more systematic process for integrating EDI in healthcare education curricula and/or programs; (2) the need to develop a digital repository of EDI-focused clinical scenarios; (3) the need for co-creating EDI-focused clinical simulations and scenarios with persons of diverse background to ensure the realistic and authentic portrayal of the respective patient population; (4) the importance of maintaining a safe learning environment for all involved persons – learners, staff, faculty and standardized/simulated patients in the EDI simulations; and (5) the need for more robust and rigorous research to advance the science of clinical simulation.
SI: development of the idea, study screening, data extraction, analysis, quality of study assessment, manuscript write-up and submission. JL: development of the idea, discuss the project idea, review and edit the manuscript. MM: literature search and manuscript review. BS: study screening, data extraction and manuscript review. NT: data extraction, quality of study assessment, manuscript review. PH: discuss the project idea, review and edit the manuscript.
None declared
None declared.
None declared.
None declared.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
Ovid MEDLINE: Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid MEDLINE® Daily and Ovid MEDLINE® <1946-Present>
| # | Searches | Results |
|---|---|---|
| 1 | Cultural Competency/ | 5958 |
| 2 | Culturally Competent Care/ | 1806 |
| 3 | cultural diversity/ | 12010 |
| 4 | Transcultural Nursing/ | 3407 |
| 5 | (cultur* adj3 (divers* or humility or aware* or safe* or competen* or sensitiv* or responsive* or congruen* or appropriate* or specific* or knowledg* or understand* or accept* or care or respect* or secur* or pluralism or expertise or skill*)).tw,kf. | 63304 |
| 6 | (transcultural or trans-cultural or intercultural or inter-cultural or cross-cultural or crosscultural or multicultural or multi-cultural or multi-ethnic or multiethnic or bicultural or bi-cultural).tw,kf. | 30192 |
| 7 | or/1-6 [Cultural Competence] | 100985 |
| 8 | simulation training/ or high fidelity simulation training/ or patient simulation/ | 10293 |
| 9 | simulat*.tw,kf. | 583409 |
| 10 | virtual patient*.tw,kf. | 1174 |
| 11 | Manikins/ | 5345 |
| 12 | (manikin* or mannequin*).tw,kf. | 5143 |
| 13 | vignette*.tw,kf. | 11831 |
| 14 | or/8-13 [Simulation] | 601213 |
| 15 | 7 and 14 | 1188 |
Embase Classic+Embase <1947 to 2021 July 21>
| # | Searches | Results |
|---|---|---|
| 1 | cultural competence/ | 7045 |
| 2 | transcultural care/ or cultural nursing/ or cultural psychiatry/ or cultural psychology/ | 5370 |
| 3 | cultural diversity/ | 2284 |
| 4 | cultural safety/ | 284 |
| 5 | cultural sensitivity/ | 1211 |
| 6 | (cultur* adj3 (divers* or humility or aware* or safe* or competen* or sensitiv* or responsive* or congruen* or appropriate* or specific* or knowledg* or understand* or accept* or care or respect* or secur* or pluralism or expertise or skill*)).tw,kw. | 81276 |
| 7 | (transcultural or trans-cultural or intercultural or inter-cultural or cross-cultural or crosscultural or multicultural or multi-cultural or multi-ethnic or multiethnic or bicultural or bi-cultural).tw,kw. | 39592 |
| 8 | or/1-7 [Cultural Competence] | 121568 |
| 9 | patient simulation/ or simulation/ or high-fidelity patient simulation/ | 200457 |
| 10 | high-fidelity simulation/ | 225 |
| 11 | simulation training/ or high fidelity simulation training/ | 6644 |
| 12 | manikin/ | 2485 |
| 13 | simulat*.tw,kw. | 638030 |
| 14 | virtual patient*.tw,kw. | 1831 |
| 15 | (manikin* or mannequin*).tw,kw. | 7656 |
| 16 | vignette/ | 6253 |
| 17 | vignette*.tw,kw. | 15334 |
| 18 | or/9-17 [Simulation] | 680027 |
| 19 | 8 and 18 | 1525 |
APA PsycInfo <1806 to July Week 2 2021>
| # | Searches | Results |
|---|---|---|
| 1 | cultural sensitivity/ | 7565 |
| 2 | cultural diversity/ | 2119 |
| 3 | transcultural psychiatry/ | 1095 |
| 4 | multiculturalism/ | 7468 |
| 5 | (cultur* adj3 (divers* or humility or aware* or safe* or competen* or sensitiv* or responsive* or congruen* or appropriate* or specific* or knowledg* or understand* or accept* or care or respect* or secur* or pluralism or expertise or skill*)).tw. | 57802 |
| 6 | (transcultural or trans-cultural or intercultural or inter-cultural or cross-cultural or crosscultural or multicultural or multi-cultural or multi-ethnic or multiethnic or bicultural or bi-cultural).tw. | 60942 |
| 7 | or/1-6 [Cultural Competence] | 110039 |
| 8 | simulation/ | 20048 |
| 9 | simulat*.tw. | 72700 |
| 10 | virtual patient*.tw. | 210 |
| 11 | (manikin* or mannequin*).tw. | 637 |
| 12 | vignette measure/ | 66 |
| 13 | vignette*.tw. | 20926 |
| 14 | or/8-13 [Simulation] | 99959 |
| 15 | 7 and 14 | 1694 |
| ID | Search | Hits |
|---|---|---|
| #1 | [mh ^“Cultural Competency”] | 182 |
| #2 | [mh ^“Culturally Competent Care”] | 100 |
| #3 | [mh ^“Cultural Diversity”] | 74 |
| #4 | [mh ^“Transcultural Nursing”] | 14 |
| #5 | (cultur* NEAR/3 (divers* or humility or aware* or safe* or competen* or sensitiv* or responsive* or congruen* or appropriate* or specific* or knowledg* or understand* or accept* or care or respect* or secur* or pluralism or expertise or skill*)):ti,ab,kw | 3479 |
| #6 | (transcultural or trans-cultural or intercultural or inter-cultural or cross-cultural or crosscultural or multicultural or multi-cultural or multi-ethnic or multiethnic or bicultural or bi-cultural):ti,ab,kw | 1264 |
| #7 | #1 OR #2 OR #3 OR #4 OR #5 OR #6 | 4549 |
| #8 | [mh ^“Simulation Training”] | 544 |
| #9 | [mh ^“high fidelity simulation training”] | 33 |
| #10 | [mh ^“patient simulation”] | 483 |
| #11 | simulat*:ti,ab,kw | 19608 |
| #12 | virtual patient*:ti,ab,kw | 9920 |
| #13 | [mh ^Manikins] | 901 |
| #14 | (manikin* or mannequin*):ti,ab,kw | 2147 |
| #15 | vignette*:ti,ab,kw | 1276 |
| #16 | #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 or #15 | 30895 |
| #17 | #7 AND #16 | 88 |
Trials = 87
((MAINSUBJECT.EXACT(“Cultural Differences”) OR MAINSUBJECT.EXACT(“Multicultural Education”) OR MAINSUBJECT.EXACT(“Cross Cultural Training”) OR MAINSUBJECT.EXACT(“Cultural Literacy”) OR MAINSUBJECT.EXACT(“Cultural Pluralism”) OR MAINSUBJECT.EXACT(“Cultural Education”) OR MAINSUBJECT.EXACT(“Biculturalism”) OR MAINSUBJECT.EXACT(“Culturally Relevant Education”) OR MAINSUBJECT.EXACT(“Cultural Awareness”) OR MAINSUBJECT.EXACT(“Cultural Context”)) OR noft((cultur* NEAR/3 (divers* or humility or aware* or safe* or competen* or sensitiv* or responsive* or congruen* or appropriate* or specific* or knowledg* or understand* or accept* or care or respect* or secur* or pluralism or expertise or skill*))) OR noft((transcultural or trans-cultural or intercultural or inter-cultural or cross-cultural or crosscultural or multicultural or multi-cultural or multi-ethnic or multiethnic or bicultural or bi-cultural))) AND ((MAINSUBJECT.EXACT(“Simulation”) OR MAINSUBJECT.EXACT(“Simulated Environment”) OR MAINSUBJECT.EXACT(“Vignettes”)) OR noft((simulat* or virtual patient* or manikin* or mannequin* or vignette*)))
Results = 1476
| # | Query | Results |
|---|---|---|
| S1 | (MH “Cultural Competence”) | 10,626 |
| S2 | (MH “Transcultural Care”) | 3,190 |
| S3 | (MH “Cultural Diversity”) OR (MH “Cultural Safety”) | 14,922 |
| S4 | (MH “Transcultural Nursing”) | 3,392 |
| S5 | TI ((cultur* N3 (divers* or humility or aware* or safe* or competen* or sensitiv* or responsive* or congruen* or appropriate* or specific* or knowledg* or understand* or accept* or care or respect* or secur* or pluralism or expertise or skill*))) OR AB ((cultur* N3 (divers* or humility or aware* or safe* or competen* or sensitiv* or responsive* or congruen* or appropriate* or specific* or knowledg* or understand* or accept* or care or respect* or secur* or pluralism or expertise or skill*))) | 37,250 |
| S6 | TI ((transcultural or trans-cultural or intercultural or inter-cultural or cross-cultural or crosscultural or multicultural or multi-cultural or multi-ethnic or multiethnic or bicultural or bi-cultural)) OR AB ((transcultural or trans-cultural or intercultural or inter-cultural or cross-cultural or crosscultural or multicultural or multi-cultural or multi-ethnic or multiethnic or bicultural or bi-cultural)) | 18,256 |
| S7 | S1 OR S2 OR S3 OR S4 OR S5 OR S6 | 67,078 |
| S8 | TI simulat* OR AB simulat* | 58,644 |
| S9 | TI virtual patient* OR AB virtual patient* | 441 |
| S10 | TI ((manikin* or mannequin*)) OR AB ((manikin* or mannequin*)) | 2,290 |
| S11 | (MH “Simulations”) OR (MH “Computer Simulation”) OR (MH “Patient Simulation”) OR (MH “Vignettes”) | 43,140 |
| S12 | (MH “Models, Anatomic+”) | 9,224 |
| S13 | TI vignette* OR AB vignette* | 5,903 |
| S14 | TI (anatom* N2 model*) OR AB (anatom* N2 model*) | 625 |
| S15 | S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 | 90,091 |
| S16 | S7 AND S15 | 892 |
((((TI=((cultur* NEAR/3 (divers* or humility or aware* or safe* or competen* or sensitiv* or responsive* or congruen* or appropriate* or specific* or knowledg* or understand* or accept* or care or respect* or secur* or pluralism or expertise or skill*)))) OR AB=((cultur* NEAR/3 (divers* or humility or aware* or safe* or competen* or sensitiv* or responsive* or congruen* or appropriate* or specific* or knowledg* or understand* or accept* or care or respect* or secur* or pluralism or expertise or skill*)))) OR AK=((cultur* NEAR/3 (divers* or humility or aware* or safe* or competen* or sensitiv* or responsive* or congruen* or appropriate* or specific* or knowledg* or understand* or accept* or care or respect* or secur* or pluralism or expertise or skill*))) OR ((TI=((transcultural or trans-cultural or intercultural or inter-cultural or cross-cultural or crosscultural or multicultural or multi-cultural or multi-ethnic or multiethnic or bicultural or bi-cultural))) OR AB=((transcultural or trans-cultural or intercultural or inter-cultural or cross-cultural or crosscultural or multicultural or multi-cultural or multi-ethnic or multiethnic or bicultural or bi-cultural))) OR AK=((transcultural or trans-cultural or intercultural or inter-cultural or cross-cultural or crosscultural or multicultural or multi-cultural or multi-ethnic or multiethnic or bicultural or bi-cultural)))) AND (((TI=((simulat* or virtual patient* or manikin* or mannequin*))) OR AB=((simulat* or virtual patient* or manikin* or mannequin*))) OR AK=((simulat* or virtual patient* or manikin* or mannequin* or vignette*)))
Results = 2109
 Equity, diversity and inclusion in clinical simulation healthcare education and training: An integrative review
Equity, diversity and inclusion in clinical simulation healthcare education and training: An integrative review
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets