Introduction
‘Physical examination of the cardiovascular system’ is one core competency a medical graduate must acquire that needs repeated practice []. Currently, these skills are being taught through facilitator-led demonstrations on healthy subjects and practice with peers []. A few challenges of the current teaching method are the paucity of subjects, lack of anatomical standardization, unwillingness by students to expose their chest in front of peers and gender-based issues []. Alternatively, simulation-based teaching using high-fidelity mannequins and simulated patients is adopted, which has been proven to be effective. The huge cost of the mannequins and the fee paid to standardized patients are felt as a major hindrance to adopting simulation-based teaching in low-resource settings []. Hence, a low-cost simulator with good functional fidelity and the necessary features to teach the skills of cardiovascular physical examination was developed.
Innovation
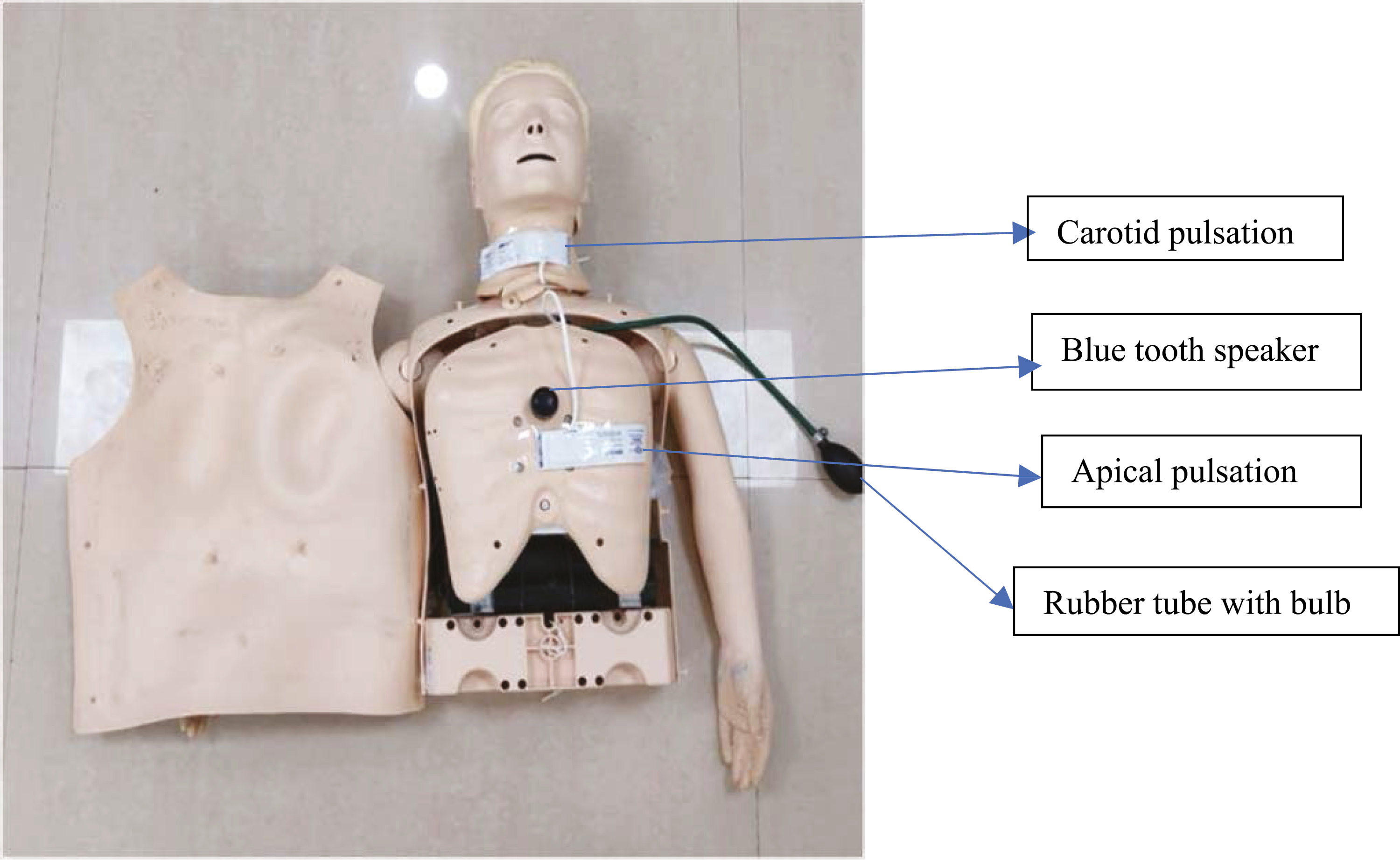
The design of the simulator (Figure 1)
- Two inflatable rectangular bladders are placed underneath the skin of a half-body mannequin, one at the location of the cardiac apex and another at the carotid triangle. A bulb is connected through a three-way connector to two silicon tubings, each of which in turn, is connected to an inflatable bladder.
- With the pumping of the bulb, the bladder gets inflated and deflated, which produces a palpable impulse through the mannequin skin, mimicking a normal apical and carotid pulsation.
- A blue-tooth speaker is placed under the precordium, equidistant from all four cardiac areas.
- Normal heart sounds are downloaded and played on a digital device connected to the speaker, which are audible when auscultated over the four cardiac areas.
Figure 1:
The design of the simulator.
Functioning of the simulator
- Palpation of apical and carotid pulsations: The bulb, which is connected to the inflatable bladder, is pressed manually at the required rate. The rate is synchronized with the heart sounds with the aid of a metronome app. Expansion of the cuff due to bulb compression creates a palpable pulsation over the chest wall and neck. It is felt by the student by placing the palm over the chest, then localized with the ulnar aspect of the hand and finally with two fingers. The manual compression of the bulb also leads to palpable pulsations at the neck, which the student locates and feels at the carotid triangle using the standard examination protocol.
- Auscultation of heart sounds: Normal heart sounds are played on a digital device connected to the Bluetooth speaker. The student can auscultate the sounds over the cardiac areas while simultaneously palpating the carotid pulsations. The heart sound that coincides with the carotid pulsation is identified as the first heart sound, and the sound that follows the pulsation is the second heart sound.
Evaluation
Faculty feedback was collected regarding the fidelity and usefulness of the model. Based on the suggestion, a few changes were made to the model for better utility in clinical examination. The cost analysis was satisfactory. The material cost of the simulator is 150 USD, whereas a high-tech mannequin with the necessary features would cost approximately 20,000 USD.
Outcomes
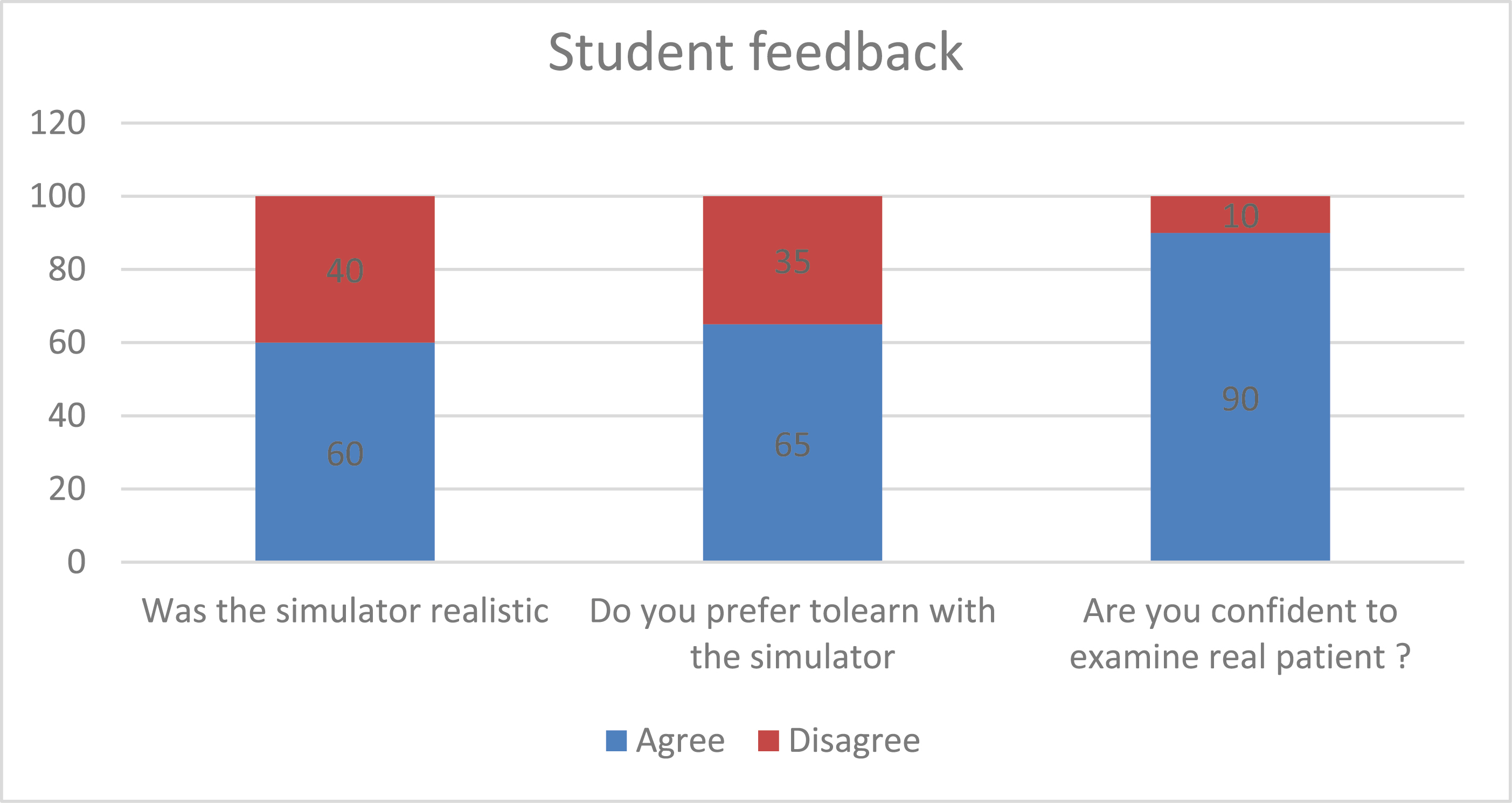
A pilot study was done to gather student perspectives about the simulator, including their preferences and confidence gained. Feedback revealed that 60% of learners felt the simulator to be realistic, while 65% of the learners preferred learning with the simulator, and 90% of the learners expressed confidence in examining real patients (Figure 2). The simulator design and functioning have been filed for a patent at the Intellectual Property Office of the Government of India [] (Auscultation, Apex Beat and Carotid Pulsation of Heart Simulator Application Number 202341018457, dated 18.03.23).
Future plan
To enhance the utility of the simulator by upgrading it to a digitally controlled motorized model with additional features such as abnormal pulsations and heart sounds, thereby promoting its applicability to teach a wider range of cardiac pathologies to advanced learners.
Authors’ contributions
None declared.
Funding
No funds received for the project.
Availability of data and materials
None declared.
Ethics approval and consent to participate
The authors declare that for this research no experiments have been carried out on humans or animals.
Competing interests
No conflict of interest and no disclosures.
References
Lekic M, Lekic V, Riaz IB, Mackstaller L, Marcus FI.
The cardiovascular physical examination–is it still relevant? The American Journal of Cardiology.
2021;
149:
140–
144.
Gowda D, Blatt B, Fink MJ, et al A core physical exam for medical students: results of a national survey.
Academic Medicine.
2014;
89(
3):
436–
442. doi:
10.1097/acm.0000000000000137. PMID: 24448049
Uchida T, Park YS, Ovitsh RK, Hojsak J, Gowda D, Farnan JM, Boyle M, Blood AD, Achike FI, Silvestri RC.
Approaches to teaching the physical exam to preclerkship medical students: results of a National Survey.
Academic Medicine.
2019;
94(
1):
129–
134. doi:
10.1097/ACM.0000000000002433. PMID: 30157090
Tuzer H, Dinc L, Elcin M.
The effects of using high-fidelity simulators and standardized patients on the thorax, lung, and cardiac examination skills of undergraduate nursing students.
Nurse Education Today.
2016;
45:
120–
125.
Tran TQ, Scherpbier A, Van Dalen J, Wright PE.
Teacher-made models: the answer for medical skills training in developing countries? BMC Medical Education.
2012;
12:
98.


 In-house designed low-cost trainer for teaching cardiovascular examination
In-house designed low-cost trainer for teaching cardiovascular examination
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets