
Learning through simulation requires psychological safety where participants feel comfortable engaging to their fullest extent, speaking up or asking questions without fear of embarrassment. While professional simulation organizations provide recommendations on fostering psychological safety, anecdotal stories from newly graduated nurses demonstrated variability in their experiences. The study explored nurses’ experience with psychological safety in their prelicensure curricula.
Using constructivist grounded theory methodology, the researchers conducted 17 semi-structured interviews with nurses who had experienced simulation in their prelicensure curriculum. They collected and analysed data iteratively using constant comparison to identify categories and explore their relationships. They used theoretical sampling in later stages until data sufficiency was achieved.
The constructed theory, Simulation Psychological Safety Ecosystem, expresses the variability of nurses’ experiences. Psychological safety is a dynamic, complex process with a spectrum of outcomes from feeling psychologically safe to suffering psychological harm. Factors that influence this outcome include clarification of Expectations, Facilitation from the instructor during scenarios, experience with Observation, and structure and quality of Debriefing/Feedback. Psychological safety is also influenced by nurses’ existing relationships with faculty and peers, and their desire to achieve meaningful clinical learning.
Implications for nursing education reinforce clarifying expectations for equipment and roles, instructor presence, and observation. The findings suggest the benefits of establishing peer and faculty relationships prior to simulation-based education implementation and providing guidelines for faculty and peer feedback. Potential areas for future research include clarifying the ecosystem model and exploring the impact of faculty and peer relationships on psychological safety.
The use of simulation-based education (SBE) in prelicensure nursing education has proliferated to include providing practice prior to clinical experiences, assessing clinical reasoning and decision-making, teaching communication skills, promoting teamwork, and increasing retention of procedural skills [1,2]. SBE is also used in prelicensure nursing education as a high-stakes assessment tool [3,4], and as a replacement for clinical hours [5,6]. One challenge that hospital-based nurse educators encounter is that new nurses sometimes are reluctant to participate in SBE due to negative prelicensure experiences. Peer-reviewed publications report nursing students describing simulation experiences as evoking negative feelings such as nerve wracking [7,8], humiliation and anger [9], and being thrown into situations unprepared [9,10]. Examining the nature of the SBE learning environment that leads to feelings of psychological safety or harm provides insight into this complex process and yields suggestions for improving SBE nursing education and guiding future healthcare simulation research.
SBE scientists adapted work undertaken by Organizational Development scholars to explicate psychological safety in the SBE environment [11,12]. The current study was guided by Turner and Harder’s concept of a psychologically safe learning environment [13]. Their definition of this concept is: ‘A … climate whereby the learner can feel valued and comfortable yet still speak up and takes risks without fear of retribution, embarrassment, judgment or consequences either to themselves or others’ [13], p. 49. In such environments, learners are willing to practise at the edge of their abilities, appreciate feedback, engage in reflection on problems and skills that are new to them, learn from mistakes, and tolerate not knowing the exact answers to complex questions [10,12,13]. If the learner experiences threats to the environment, they may not fully engage with the simulation, question the realism of the simulation or technology, feel exposed by the simulation and/or debriefing in a way that can threaten their professional identity, or feel defensive discussing performance that falls short of a standard and subsequently miss the recognition of the error and the potential for correction [12–14]. Since psychological safety promotes skill acquisition, knowledge gains and problem-solving ability, several simulation experts and professional organizations such as the Society for Simulation in Healthcare (SSH) and the International Nursing Association for Clinical Simulation and Learning (INACSL) have provided recommendations on how to promote optimal learning environments.
Recommendations for promoting psychological safety offer best practices for prebriefing, debriefing and facilitator characteristics. Prebriefing recommendations include clarifying objectives; environment and equipment functionality; roles of the participants and faculty, confidentiality of the session and expectations of the learners; establishing a ‘fiction contract’ with the learners to act as if things are real in order to gain the maximum amount of learning from the time in the scenario; attending to the logistical details of the session; and conveying a commitment to respecting learners and understanding their perspective [12,15,16]. Debriefing practice recommendations for achieving a safe learning environment include debriefing led by a competent facilitator who actually observed the scenario, using a structured debriefing framework, using evidence-based facilitation techniques, and providing an environment that supports trust, confidentiality, and self-reflection [17–19]. Facilitator characteristics can greatly influence psychological safety, and some desired attributes include positive attitude, calm demeanour, knowledge of simulation pedagogy, ability to provide prompt feedback, ability to identify gaps in knowledge and skills, and the ability to integrate clinical standards into scenarios [20,21]. Although recommendations for promoting psychological safety in SBE are readily available to educators, they are not mandated in the United States by regulatory agencies for nursing academic institutions or state boards of nursing.
Despite recommendations for creating psychological safety, reports of distress during prelicensure nursing simulation persist in the literature [7,9,10] and in anecdotes. The purpose of this study was to explore nurses’ experience of psychological safety during simulation in their prelicensure programmes. The research question for this study was: What was the nursing students’ experience of psychological safety in the SBE learning environment?
In SBE, learning often occurs in small groups as a social practice [22]. For that reason, the Constructivist Grounded Theory (CGT) approach was chosen as it focuses on an interpretive understanding of a social phenomenon, models that are specific to situated circumstances, and reflects the philosophical worldview of the first researcher (S.E.) [23,24].
Reporting standards for qualitative research publications specify that researchers disclose ways in which their experiences might influence their interactions with participants or the data [25]. The topic was informed by researchers’ (S.E., T.L.H.) various positive and negative anecdotal stories from nurses’ prelicensure simulation gained during over 35 years of combined experience in SBE. The researchers’ reflexivity for this research project entailed acknowledging the influence of the various experts on their perspectives and balancing that with the sacred task of honouring the nurses’ stories while constructing the theory. Three of the four researchers (S.E., F.V., J.C.) have previous experience using classical grounded theory as a qualitative method.
CGT, based on extracting data from a unique social group, requires purposive sampling [23,26]. Inclusion criteria for participation: Nurses who had graduated from nursing schools during the last 24 months and who experienced in-person SBE in their prelicensure curricula were currently working in an acute care setting and spoke English. Nurses who had experienced only online or virtual simulation were excluded.
Sample size for CGT is not determined by any statistical power, but by reaching the point of theoretical sufficiency where the researchers were not obtaining any new data that might indicate the need for additional categories. Recruitment for this study was initially done by distribution of Information Sheets (see Supplemental Digital Material A) to nurses meeting the inclusion criteria by hospital-based educators known to the researcher from various simulation professional organizations. Recruitment was also accomplished by the ‘snowball’ [27] technique of asking participants if they know others who might like to participate. Participants who completed the interview were given a $10 Starbucks gift card in appreciation for their time.
Seventeen interviews were conducted with participants who had graduated from nursing schools within 24 months. The interviews occurred in three different rounds: September through November of 2020, September through November of 2021 and May of 2022. Table 1 outlines demographic information obtained from the participants and their assigned pseudonyms. All 17 of the nurses reported using mannequin-based simulation and task trainers during their prelicensure curriculum. An additional eight reported using simulated patient methodology, seven described also using role play and one reported using virtual reality as a pilot programme. Another screening criterion was that nurses experience SBE for learning and not just testing, so all 17 reported learning and 6 reported some type of assessment. One potential area of exploration was psychological safety for high-stakes assessments; however, none of the six experienced high-stakes exams, just SBE exercises that were graded for participation and clinical reasoning.

| Pseudonym | Gender | Age range | Ethnicity | Type of nursing programmes and location |
|---|---|---|---|---|
| ‘Lei’ | Female | 25–34 | Asian | ABSN, Washington DC |
| ‘Kai’ | Male | 18–24 | Asian | BSN, San Francisco |
| ‘Ivy’ | Female | 25–24 | Caucasian | MSN Entry, Sacramento |
| ‘Sophia’ | Female | 18–24 | Hispanic | BSN, San Jose |
| ‘Maya’ | Female | 18–24 | South Asian | BSN, Los Angeles |
| ‘Emma’ | Female | 18–24 | Caucasian | BSN, San Francisco |
| ‘Julie’ | Female | 25–34 | Caucasian | ABSN, Sacramento |
| ‘Javier’ | Male | 25–34 | Hispanic | MSN Entry, Boston |
| ‘Valerie’ | Female | 18–24 | Caucasian | ABSN, Springfield (MO) |
| ‘Bailey’ | Female | 18–24 | Caucasian | BSN, Boston |
| ‘Amy’ | Female | 25–34 | Caucasian | MSN Entry, Chicago |
| ‘Priya’ | Female | 18–24 | South Asian | BSN, Chicago |
| ‘Tessa’ | Female | 25–34 | Caucasian | MSN Entry, Chicago |
| ‘Rebecca’ | Female | 18–24 | Caucasian | BSN, Normal (IL) |
| ‘Sabrina’ | Female | 18–24 | Caucasian | BSN, Normal (IL) |
| ‘Jade’ | Female | 25–34 | Asian | MSN Entry, Chicago |
| ‘Molly’ | Female | 25–34 | Caucasian | ABSN, Miami |
Notes: ABSN = Accelerated Bachelor of Science in Nursing; BSN = Bachelor of Science in Nursing; MSN = Master of Science in Nursing.
This research was approved by the Loyola University Chicago Institutional Review Board (213702). Data collection took place via Zoom audio-recorded interviews that lasted between 24 and 50 minutes using the interview guide (see Supplemental Digital Material B) that included the purpose of the study, some demographic information and semi-structured interview questions. All interviews were conducted by researcher S.E. Once the interviews were completed, the recordings were assigned a randomly generated code number and then sent securely to a certified CITI-trained transcriptionist. Transcripts were reviewed for completeness and lack of identifiers, and then researcher S.E. uploaded them into NVivo 20 software (QSR International, Melbourne, Australia) using the randomized code number and assigned a pseudonym. Researchers (S.E., F.V., J.C.) used transcripts of the recorded interviews and handwritten field notes to clarify data, guide further discussion with the participants and capture suggestions for subsequent interviews [23,26].
In CGT, data collection and analysis occur concurrently via constant comparison, which allowed researchers to identify similarities and differences that shaped the emerging categories and their properties [23,28]. The procedure for CGT followed the steps of initial coding, focused coding, theoretical sorting, diagramming and integrating. Initial coding by two researchers (S.E., F.V.) involved systematic examination of data line by line throughout the transcript and creating codes based on participants’ words [23,29]. In focused coding, emerging codes were examined by researchers (S.E., F.V., J.C.) to determine ones that appeared frequently or had more significance [23]. Once conceptual categories were identified, their meanings were clarified in memos. The next step was tabling and diagramming visual representations of the categories and their relationships to each other [23,28]. Examining the relationships between the conceptual categories, reviewing the memos and transcripts and developing the visual model led to the construction of the core category Simulation Psychological Safety Ecosystem. The researcher group constructed the theory utilizing the identified core category, key factors, and relationships detected in the data and memos.
Charmaz [24] asserts the purpose of theoretical sampling is not to increase the size of the sample but rather to refine ideas and themes that have already emerged in the initial coding. For this study, the theoretical sampling involved refining the interview questions based on nurses’ suggestions to explicitly ask about nurses’ relationships with faculty and peers to determine how that impacted their feelings of psychological safety (see Supplemental Digital Material C). Data collection ended after the factors were sufficiently explored.
An established criterion for trustworthiness consists of credibility, transferability, dependability and confirmability [30]. CGT provided credibility in that the researcher used the participants’ words as the data for analysis; maintaining records of the transcriptions allowed the researcher to have verifiable access to those data. The researchers actively engaged the participants in co-constructing the data by sending interested participants the substantive theory to seek verification and corrections. Transferability to other contexts was achieved in this CGT study by the thick descriptions described in the participant data and by selecting participants from a variety of geographic locations. Comparing codes between researchers (S.E., F.V., J.C.) provided dependability. Confirmability for the study was enhanced using memos and audit trails throughout the open and focused coding process, and by performing member checking with interested participants via email after the theory was constructed.
The theory conceptualized and constructed from the nurses’ data is depicted in Figure 1. The core category Simulation Psychological Safety Ecosystem refers to the myriad of experiences the nurses have in prelicensure simulation based on the interplay of the factors. The theory consists of four major factors that influence nurses’ experience of psychological safety: Expectations, Facilitation, Observation and Debriefing/Feedback. Each of these factors has sub-factors along a spectrum of impact on the nurses. Labels were constructed to describe these spectrum dimensions: Promoters of Psychological Safety describes when factors allow nurses to feel that they can learn and make mistakes without being embarrassed; Barriers to Psychological Safety describes when various factors cause ambiguity in nurses’ sense of safety; and Causes of Psychological Harm expresses when individual or combined factors cause nurses to feel unsafe in the SBE environment. Nurses’ experience of psychological safety was also influenced by their existing relationships with faculty or peers and their perception of whether the simulation was meaningful to their clinical practice.

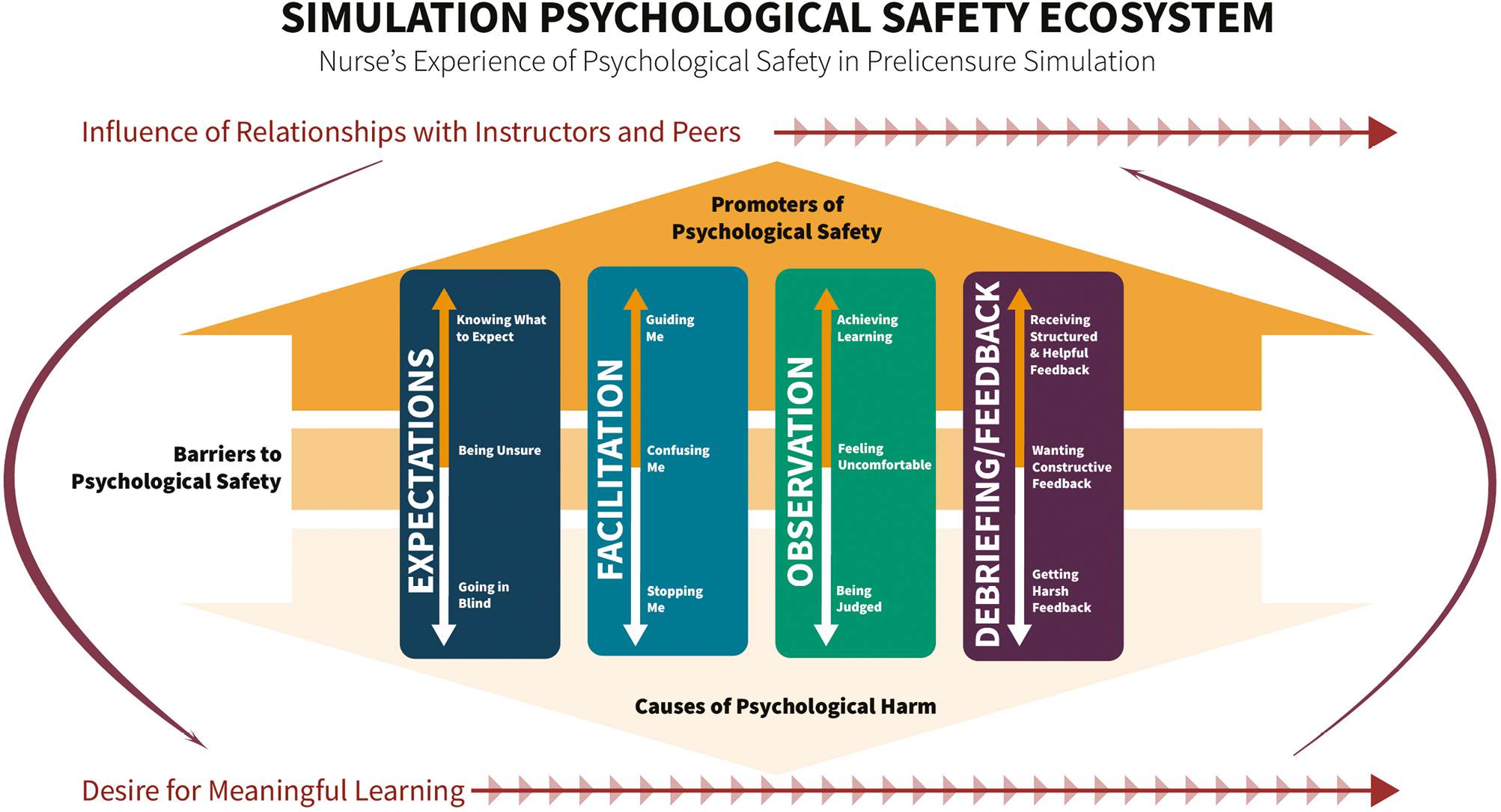
Simulation psychological safety ecosystem: nurses’ experience of psychological safety in prelicensure simulation
The complexity and interactivity of factors with the mediating variables drove the choice of terminology for the core category, shifting from the term and concept of a psychologically safe environment to psychological safety ecosystem. The term ecosystem originated in the discipline of ecology to describe the intertwined nature of living organisms and their environments [31]. The term has been adapted in the education discipline to describe complex interdependent factors as learning ecosystems [32]. Ecosystems can be altered by fluctuations in the nutrient cycles that provide sustenance and the flow of energy through the system [31]. In this model, the factors represent the nutrient cycles, as they are based on explicit behaviours from the instructors and learners; and the mediating variables represent the energy flow through the system, as they are based on implicit stimuli. While these factors are not linear, the visual model depicts them in the order that the nurses encounter them empirically within their experiences. Tables 2 and 3 utilize tabular format for qualitative research [33] to provide concise descriptions of factors and sub-factors with illustrative quotes from the participants.
| Factors and sub-factors | Description | Sample nursing quotes |
|---|---|---|
| Expectations | ||
| Knowing what to expect | Familiarization to the environment, roles, and ground rules helped nurses engage with the simulation | We were very well prepped for what was going on in the room. They showed us where the medications and supplies were kept … we were familiar with everything (Molly) They would read the goals of sim and then say that we believe you can do your best and deserve to be supported (Rebecca) |
| Being unsure | A lack of clear expectations led to feelings of uncertainty | We went in there and had no idea what was going on … we were just bumbling around – it was very unproductive (Emma) They did not tell us the goals … maybe 15 minutes later if we said what they wanted they would stop the sim (Kai) |
| Going in blind | Going in blind inhibited participation and caused nurses to dislike SBE | They didn’t tell us the goals of the sim … and I walked in to a mannequin squeezing out a baby head and screaming in pain. Going in so blind with such little data ... is just kind of paralyzing (Julie) Going in blind felt like a spotlight was on me … I was ready to be exposed for not knowing or doing the wrong thing … it took up so much mental energy (Jade) |
| Facilitation | ||
| Guiding me | Instructor presence in the simulation room promoted security by having someone who could assist if needed | The midwife was in the room … and went through all the positions and therapeutic measures we could offer the patient (Lei) Rather than let us fumble around … he (instructor) was like, I’m going to be in the corner of the room, I am going to be with you, it’s going to be okay (Ivy) |
| Confusing me | Lack of instructor presence or guidance caused nurses to feel stuck | You wouldn’t really get extra help if you stumbled … it was kind of like you are on your own (Julie) You don’t have to walk us through it … but it would be good to get hints, especially if it is going off course (Sabrina) |
| Stopping me | Being interrupted during scenario caused harmful feelings of being frozen or unable to continue | I went to administer the medication and she grabbed my arm, stopping me … it was pretty intimidating (Bailey) She would interrupt us during the middle of the sim, we were afraid to move forward because we were not sure when she would interrupt us again (Molly) |
| Description | Illustrative quotes | |
|---|---|---|
| Observation | ||
| Achieving learning | Nurses expressed benefits from watching their peers go through scenarios and having instructions for observing | As a viewer it was very informative because we are able to learn from four scenarios while only being an active participant in one (Tessa) As observers, we were told to write down a few things that you thought went well and a few things you thought they might change (Priya) |
| Feeling uncomfortable | Nurses experienced insecurity when they were unclear on observation roles or how they were perceived | The other students were sitting in a room – maybe judging me, maybe not judging me, and the clinical instructor is doing the same. I was not a fan of that (Amy) |
| Being judged | Having peers or instructors laughing or yelling while observing caused psychological harm – especially if nurses heard during the scenario | We would be yelling at the screen in the observation room. ‘Look at the vitals – they are about to code – what are you doing?’ (Kai) Being in the simulation and knowing that someone is watching you … sometimes you can actually hear the yelling (from the instructors or peers) … and it makes you think what am I doing wrong? (Sophia) |
| Debriefing | ||
| Receiving helpful/structured feedback | Supportive structure and debriefing techniques allowed nurses to feel safe | Usually when we’d come back, we’d always talk about what we did good first, which I thought was very helpful (Molly) What I found super helpful was when we discussed things that were noticed amongst the group and not as an individual … it felt more comfortable to learn because they wouldn’t mention one person (Javier) I knew if I made a mistake, we could talk it through in the debrief afterwards and I wouldn’t be penalized for it (Jade) |
| Wanting constructive feedback | Nurses were frustrated if they did not receive feedback that was designed to help them improve | Our instructor encouraged us to say one thing, but sometimes it was just a fluffer (Lei) You want to give positive feedback to everyone, but at the same time you wish you could get some of that other (constructive) feedback (Sophia) |
| Getting harsh feedback | Nurses became frightened, angry or defensive when either they or their peers experienced harsh feedback | He barely said good things – just this was wrong and that was wrong … but didn’t explain what was wrong about it – you just feel bad (Emma) My instructor was so nit-picky on those tiny (negative) details … as opposed to the bigger picture – clinical decision making (Ivy) |
All participants described how variability in knowing expectations contributed to their sense of psychological safety. Nurses expressed more willingness to fully engage in SBE when they were familiar with objectives, environment and equipment, roles of the participants, logistics, confidentiality, and any evaluation. Not knowing what to expect was a frequent source of anxiety or embarrassment for nurses. The variability of when, how and to what extent this information is delivered was one of the most prevalent themes discussed by the nurses. The sub-factors for this category along the dimensions were Knowing What to Expect, Being Unsure and Going in Blind.
This factor describes participants’ stories of how the actions or presence of their instructor during the scenario impacted their sense of psychological safety. Participants felt less fear of making mistakes when they knew their instructor would provide guidance as needed during the scenario. Nurses experienced angst when instructors disrupted the flow of the case without explanation. The sub-factors for this category along the dimensions were Guiding me, Confusing me and Stopping me.
One of the most frequently mentioned factors was being observed by faculty and peers. Sometimes instructors were present in the simulation suite; other times they were watching from an attached control room, usually with a window or mirror. Due to the size of simulation groups within nursing schools, there were usually some active participants in the scenario and some additional learners watching from a remote location. Being observed usually caused at least some discomfort for the nurses and was a source of psychological harm when the nurses described being yelled at during observation by either faculty or peers. The sub-factors for this category along the dimensions were Achieving learning, Feeling uncomfortable and Being judged.
Debriefing is one of the key functions of learning in the simulation process, especially when the participants feel safe discussing their behaviours, identifying gaps in performance and discovering opportunities for future improvement. The participants’ data reinforced the value of psychologically safe debriefing for their learning and described ways in which the structure of debriefing and nature of feedback influenced that variable. Nurses verbalized that learning during the debriefing increased their comfort and allowed them to perform better in subsequent simulation scenarios. Many of the challenges to psychological safety were concerns regarding the quality and nature of feedback provided. The sub-factors for this category along the dimensions were Receiving structured and helpful feedback, Wanting constructive feedback and Getting harsh feedback.
Another part of the model is that there were also a couple of underlying variables that could influence the nurses’ overall sense of safety and how the various factors interact to produce psychological safety, ambiguity or psychological harm. These pre-existing variables, detailed with quotes in Table 4, were the influence of relationships that nurses had with instructors and peers, and their desire for meaningful clinical learning. The variables’ impact mirrored an ecosystem where the energy flow is typically unidirectional but can be altered by fluctuations to the environment or organism [31].
| Mediating variable | Description | Sample nursing quotes |
|---|---|---|
| Desire for meaningful learning | Nurses reported part of feeling psychologically safe during SBE was having scenarios that were relevant to their future clinical work – either for school rotations or current clinical role | I remember having really good ones, just like practicing CPR with everybody and practicing lateral violence and bullying in the workplace. Those were great simulations that I found very helpful and supportive (Lei) I think that simulation offers … chances to work out the kinks in, from just transferring over what you’ve learned in school to actually putting it into work, like into practice. And for me, that was always the best way I learned when I learned something, physically performed it or executed it and then it would just stay with me much longer (Bailey) |
| Influence of relationships – instructors | Positive existing relationships with instructors alleviated fears of making mistakes since the nurses did not feel they were being judged solely on one scenario. Negative relationships with instructors increased nurses’ anxiety around being observed and receiving harsh feedback | If it was your own clinical instructor, they kind of know you better and so that generally produced a better result … if it was someone that I had never had as a teacher before or something like that, then I felt like they were a little bit more cold and hard to warm up to (Sabrina) I didn’t necessarily have the best relationship with that clinical instructor that term as well. So, for me, I guess I’m going into it already in kind of an upset situation (Ivy) |
| Influence of relationships – peers | Some of the nurses reflected they had not realized the impact of previous relationships with peers until being interviewed. They indicated greater psychological safety when they had positive existing relationships with peers or having time or opportunities to know them better | It really depends on how someone views that scenario based on how well they know their classmates … for people who didn’t have good relationships with them or good rapport with them, it was a very, very stressful scenario versus someone, a group of eight who maybe who had a really close knit, it was just like a normal day hanging out with some close friends of theirs. So, I think it really depended (Tessa) I had very amenable relationship with my classmates and it’s easy to give more criticism, again when you’re not in that stressful scenario. You just choose to be respectful of course. But I think that a friend who was recently in this scenario, she was telling me about another classmate who was verbally snickering and saying oh that’s so silly, like oh why did they do that, just very noticeably making it a comical scenario and she was kind of upset by that (Jade) Having everyone watch was extremely nerve-wracking. And I think one piece of it was the first few times doing it, the first few, first semester really was nerve-racking because you’re like oh, are these people going to judge me? … And then in consequent simulations, we all, we got to know each other. And so, you’d come out and people will be supportive, and that was really nice (Priya) |
From the first interview, one of the topics that emerged was that instructor presence during simulation, observation by instructors and peers, and feedback were all influenced by nurses’ existing relationships. Having previous positive or negative relationships with faculty and peers affected psychological safety, especially nurses’ willingness to actively engage in simulations where they might make a mistake. Hearing about this phenomenon led to changing the interview questions and theoretical sampling to purposefully explore this relational aspect of psychological safety in prelicensure nursing simulation.
Another influencing theme from many of the nurses was that for them to feel that SBE was a safe environment, they wanted it to have relevance to their future clinical work, either for school rotations or their current occupation. They appreciated how the experiential SBE could prepare them for practice and expressed frustration if they felt it was not useful. This variable highly interacts with the nurses’ desire for constructive feedback since many expressed that they were told they could make mistakes and learn from them, but then were not given guidance on how they could improve their knowledge or skills.
The theory Simulation Psychological Safety Ecosystem describes the factors that can contribute to nurses feeling comfortable participating to their fullest, making mistakes without fear of embarrassment and speaking up. The dimensions of Promoters of Psychological Safety, Barriers to Psychological Safety and Causes of Psychological Harm depict the range of psychological safety nurses encountered and can be altered by the nurses’ interaction with the four main factors and mediating variables. Ecosystems thrive when alignment exists between the organisms and the environment, and strong fluctuations can positively or negatively impact the resilience of the system [31,32]. The simulation psychological safety ecosystem reflects this interdependency via the overlap and interplay between the factors that can also be influenced by mediating variables such as nurses’ previous relationships with instructors or peers. This ecosystem model is consistent with Kolbe et al.’s [34] assertion that ‘psychological safety is not stable, but rather a dynamic and fragile perception’ (p.165) that depends on the interaction of various factors. Purdy et al.’s [35] recent work on the ‘Leaky Container’ reinforces the energy flow within the psychological safety ecosystem, as it describes how existing relationships can reciprocally shape psychological safety in SBE and exterior settings.
Psychological safety in prelicensure nursing has been a rising topic, with four qualitative studies published during the data collection and analysis phase for Simulation Psychological Safety Learning Ecosystem [36–39]. These and other studies reinforced the various factors and mediating variables within the model, The Expectations factor recurred in Kostovich et al.’s [36] theme of Setting the stage and in Kang and Min’s [10] theme of Feeling Unready. Facilitation impact on psychological safety appeared in Stephen et al.’s [38] Faculty Presence and Kostovich et al.’s [36] Planned Strategies. The anxiety that nurses experience from Observation by faculty and peers has recurred throughout nursing SBE literature[10,38–40]. Debriefing/Feedback is perhaps one of the most studied aspects of SBE, and there are several recommendations for achieving psychological safety in the literature [10,34,39,41,42]. Relationship variables for psychological safety are supported by findings that students perceived greater psychological safety with faculty who knew them and were aware of their clinical abilities [39], and modified their participation and behaviour in simulation based on what they knew about the professor [37]. The peer variable was echoed in Stephen et al.’s [38] Working together theme where nurses preferred to be in scenarios with those that they knew were equally committed to learning. Park and Kim’s [37] study raised similar concerns in their theme Dangers of team dynamics—namely, that having trusting relationships with their peers promoted psychological safety, and not knowing them caused psychological risk and fear of participating and giving feedback. The factors and mediating variable findings suggest improvements for SBE in prelicensure nursing.
CGT has an inherent limitation because it is designed to describe phenomena within a limited context, and not generalizable. Recruiting nurses via nurse educators may have some social desirability bias in that the new nurses wanted to please their preceptor/educator. One recruitment goal was to gather data from a variety of educational programs and the information sheet was sent to several organizations and institutions to achieve this goal. However, due to the nature of the first researcher’s network, the respondents mostly came from U.S. institutions where a BSN is the entry level for hiring, so there were no Diploma or Associate Degree graduates in the sample. One goal of this study was to assess psychological safety during high-stakes assessment; however, none of the participants experienced that during SBE. The six nurses who reported assessment with SBE were given class points for participation and accuracy of clinical reasoning and actions taken. The only reported challenge from two participants was not having clear expectations of point scales. Another limitation of this study was that data collection was delayed several times due to the global pandemic. Nurses in later rounds had more time pass since they graduated from nursing school, creating a potential for recollection bias.
The genesis for this study was provided by challenges reported during nursing prelicensure simulation, and despite numerous professional guidelines and standards, SBE continues to be a source of distress to nurses. In addition to the qualitative studies mentioned above, a recent social media post regarding the SSH Nursing Interest group discussed how negative experiences persist in prelicensure SBE [43]. Over 50 nursing educators gathered to comment and discuss how best to ameliorate the challenges to prelicensure SBE psychological safety. Negative emotional experiences can cause learners to remember only the emotions and not the clinical reasoning, communication or other skills that were intended [14]. Ensuring psychological safety and quality debriefing allows learners to process their mistakes and learn instead of focusing on embarrassment.
One challenge remains ensuring adequate faculty development in SBE best practices. The INACSL Healthcare Simulation Standards Endorsement programme recognizes institutions that have achieved excellence in four standards: Prebriefing, Facilitation, Professional Integrity and Debriefing. These four standards align with the four factors within Simulation Psychological Safety Ecosystem . INACSL [44] and the National Council of State Boards of Nursing [45] provide guidelines for providing psychologically safe learning environments which should be accepted standards for use of SBE in prelicensure nursing curricula. Despite nursing and simulation organizations recommending specialty certification for SBE educators, recent literature demonstrates that up to 71% of SBE facilitators in U.S. prelicensure programmes did not have the certification even though they were using SBE to replace traditional clinical hours [46,47]. SBE is firmly entrenched in prelicensure curricula and faculty should have both the training and the desire to utilize this form of education.
Faculty qualifications in SBE are necessary, but not sufficient, for psychological safety based on nurses’ emphasis of the impact of their previous relationships with faculty and peers. Since nurses report enhanced safety engaging in SBE when they have established relationships with faculty, nursing schools should ensure that students have been introduced to the faculty and avoid having random faculty assigned to facilitating exercises. Ideally, instructors and other simulation team members should be introduced to participants before SBE exercises. The interview guide was modified based on nurses’ recognition that their peers had a significant influence on their perceptions of psychological safety. Nurses expressed that having set cohorts where they had consistent groups for SBE during a semester positively impacted their sense of safety. The nurses valued the incorporation of icebreakers if they had not met instructors or peers prior to SBE, as Valerie indicated ‘it is really nerve wracking ... is this going to be the impression that I have on someone forever?’ Another recommendation for nursing education would be to consider these ameliorating techniques so that nurses feel safer speaking up, making mistakes or performing to their fullest extent.
The challenge to psychological safety from observation in SBE deserves focused attention in nursing education. Best nursing educational practice should follow the latest Healthcare Simulation Standards of Best PracticeTM , which stipulate that part of the prebriefing should include providing information regarding the use of recording and observations by peers, faculty and staff [15]. Faculty should also establish ground rules for observation that would mitigate negative peer behaviours, such as yelling or snickering at the screen found in this and other studies of prelicensure nursing SBE [38,40]. Another suggestion is directed observation, where participants have observer role clarity, use tools to focus attention and participate in the debriefing [48].
Another interesting implication from this study was the nurses’ desire for more constructive feedback from their peers and instruction on how to provide that feedback:
… it is kind of an uncomfortable situation to be in to give feedback to your peers because you don’t want to offend them. But I think it’s an important skill to have. It is a skill that would be useful to have forever, so I wish they had given us instruction on it (Rebecca).
One technique that nurses could easily be taught is how to give directive feedback. This technique entails giving an observation of a behaviour, a suggestion for change, a rationale for the change and an invitation to discuss [49]. Teaching this structure to nurses and allowing them an opportunity to practise using it in a mentored situation during SBE would give nurses a useful skill that translates to their clinical practice. Providing constructive feedback enhances participants’ sense of achieving meaningful learning.
An initial goal for this study was to potentially utilize the theory to develop an instrument to measure psychological safety. However, explicating psychological safety as an ecosystem is a novel conceptual model that requires future exploration of how the various factors interact, if personal characteristics of simulation participants might influence their perceptions, and what impact existing relationships have on psychological safety. Refining the theory would include future qualitative work to explore some of these nuances. This study purposefully focused on nurses’ perceptions of psychological safety and the resulting theory describes that phenomenon. Recent literature demonstrates that there are differences in student and faculty perceptions [36,38,39]. Since psychological safety is intended to be a property of the learner in SBE, and not the faculty [34,39], future research should explore the gaps that may affect how faculty construct psychological safety in prelicensure SBE.
The authors would like to acknowledge Dr. Bec Szabo and Kirsty Freeman for identifying that the core category of psychological safety is best represented by the term ‘ecosystem’. Thank you to Derek W. Wade and Deila Bumgardner, who assisted in translating the theoretical model into the current graphic depiction.
S.E., F.V. and T.L.H. made substantial contributions to the rationale and design of the study. S.E., F.V. and J.C. analysed the data and interpreted results. S.E. drafted the manuscript. All authors commented on each draft of the manuscript. All authors read and approved the final manuscript.
No funding has been received for this research.
None declared.
This research was approved by the Loyola University Chicago Institutional Review Board (213702), and written informed consent was obtained from all participants.
None of the authors have financial interests to declare.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.

 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets