Simulation centres across the world are increasingly being recognized as pivotal in health profession education. More than just physical space to locate learning, they should also be a space and place that enhances learning. The built and physical environment of a simulation centre has the potential to further enhance educational dynamics. Despite the importance of such resource-intensive settings for learning, how the built environment can help shape learning (i.e. built pedagogy) in simulation centres is a much-neglected entity. This essay explores how learning theories may be used to shape the design process of a health professions simulation centre. Drawing upon our experiences of being involved in the design of a simulation centre and the importance of social interactions on learning, we discuss how sociocultural learning theories may guide this process, and positively influence the physical design and build of a simulation centre.
What this essay adds
Simulation can be a force for good. In creating simulated realities, we have the potential to transform learners and for learners to transform the world around them. This is nowhere more evident than in healthcare simulation-based education. Healthcare simulation practice has no physical boundaries per se, whether situated in authentic work locations (‘in situ’ simulation) or in bespoke simulation centres. Simulation centres can offer a defined space for teaching across the learning spectrum; from novices – to more experienced practitioners. They are, or rather they should be, more than merely physical spaces in which learning is located, but should additionally be spaces that enhance learning. They have the potential to promote individual agency and enhance educational dynamics. By the careful design and construction of the physical place in which the simulated learning occurs, there is potential to positively influence the knowledge, behavioural and skills outcomes of the learners in that space. Having been recently involved in the design of a new simulation centre, we became very aware of the scarce published information to best guide and inform how to best influence the design and build of the physical environment in simulation centres to shape learning (i.e. built pedagogy).
In this essay we consider how learning theory can be used to shape the design process of a health professions simulation centre. We draw upon sociocultural perspectives to consider the design process and also how pedagogical theory can usefully inform the design and physical environment of a simulation centre. We provide some examples from our own experience in the design of an interprofessional simulation centre, KN Cheung SK Chin InterSim Centre (InterSim), at Queen’s University Belfast.
Designing a new simulation centre can be an exciting, but challenging activity. For any health professions educational institutions, a simulation centre can help transform the professional skills of learners, create collaborative learning opportunities and manifest a valued commitment to education – but at considerable cost. Simulation centres are expensive facilities in terms of capital costs, equipment, staffing and ongoing running costs. Their design needs to be a thorough and measured process. Crucially the educational purpose of the centre must never get lost in this design process; otherwise, the centre is at risk of not fulfilling its educational objectives.
Education faculty staff often have limited, if any, experience in designing a simulation centre. However, they are knowledgeable about simulation-based education delivery and they are the staff who will inhabit the centre and deliver its activity on build completion. While professional design teams are essential in providing expert guidance, their collaboration with faculty staff in the design process is key. Dialogue between the faculty staff and design team should help to refine and enhance the final product. As in all working relationships, there can be synergies and tensions, and with the resolution of such tensions, transformation and growth. Values such as criticality, integrity and compromise are important to such working relationships (i.e. tensegrity – a neologism of ‘tension’ and ‘integrity’) and provide optimal conditions for the design process. Design teams need to closely engage with relevant faculty staff to develop an understanding of the needs and functionality of the simulation centre. Simulation centres are not mere replicates of clinical environments – they are built spaces, informed by clinical environments, to promote effective learning.
For many educational faculty staff, building a new simulation centre is a once in a career opportunity. It is a highly complex activity with multiple elements and a bewildering range of influences. From a sociocultural stance, Culture Historical Activity Theory (CHAT) is a lens that can help conceptualize complex human activities such as the design of a simulation centre (see Figure 1) [1]. CHAT affords an analytical tool to consider and guide the various elements, and mediating factors, involved in this design activity.

![Diagrammatic representation of Culture Historical Activity Theory of a human activity [1].](/dataresources/articles/contents-1666857948204-9be5661e-7dfe-4ea7-a767-89ad80c354e2/assets/ijaa051f0001.jpg)
Diagrammatic representation of Culture Historical Activity Theory of a human activity [1].
First, there has to be a desired purpose, or product, of this human activity (i.e. object ) – for example, designing a simulation centre that provides the best educational opportunity for learners (see Figure 2).
![Diagrammatic representation of Culture Historical Activity Theory as applied to the design of a simulation centre [1].](/dataresources/articles/contents-1666857948204-9be5661e-7dfe-4ea7-a767-89ad80c354e2/assets/ijaa051f0002.jpg)
Diagrammatic representation of Culture Historical Activity Theory as applied to the design of a simulation centre [1].
This object-oriented action will require key individuals (i.e. subjects) to invest effort in achieving this object. They are agents – who will take an active role in producing change. The object holds the community together and gives it a long-term purpose. In the context of designing a simulation centre, this will include simulation practitioners and professional support staff who will ultimately inhabit and run the centre. Such subjects will utilize mediating instruments (i.e. tools and artefacts) in this design process. For example, developing 3D models (Figure 3) of a proposed design or a design ‘mood-board’ with images and ideas from other simulation centres.

Example of ‘mediating instruments’ (VR headset and 3D model) to review proposed plans of a new simulation centre.
In addition to subjects, objects and mediating instruments – there are other social mediating elements in any human activity system, i.e. rules, community and division of labour. Rules refer to regulations that govern the activity. In the design of a simulation centre, there will be a wider range of procedures that need to be adhered to – for example, building regulations, projected educational usage of the centre and capital budgetary limits. Beyond the subjects, there will be a number of individuals and groups who will have vested interests in the centre (i.e. community ). They form the social context and network for the centre (Figure 4). Finally, within the activity system of designing a simulation centre, there will be social structures that determine responsibility for particular actions (i.e. division of labour). In our process, for example, we decided that key educational faculty staff from various subject disciplines research other simulation centres and present this to the design team.

‘Community’ of learners, simulated participants and patient steering group in the design of the InterSim simulation centre.
Between these various elements of the design activity, invariably there may be tensions (or contradictions). For example, during our process the faculty staff (subjects ) considered that the design should be more hospital-centric but other important stakeholders (from our community of health practitioners) expressed the need to have more primary care environments (consultation rooms and a home environment) represented in the simulation centre design. Resolution of these contradictions ensures that progress is made in designing a simulation centre best suited to the specific object needs. Figure 5 diagrammatically represents this design process, informed by CHAT.
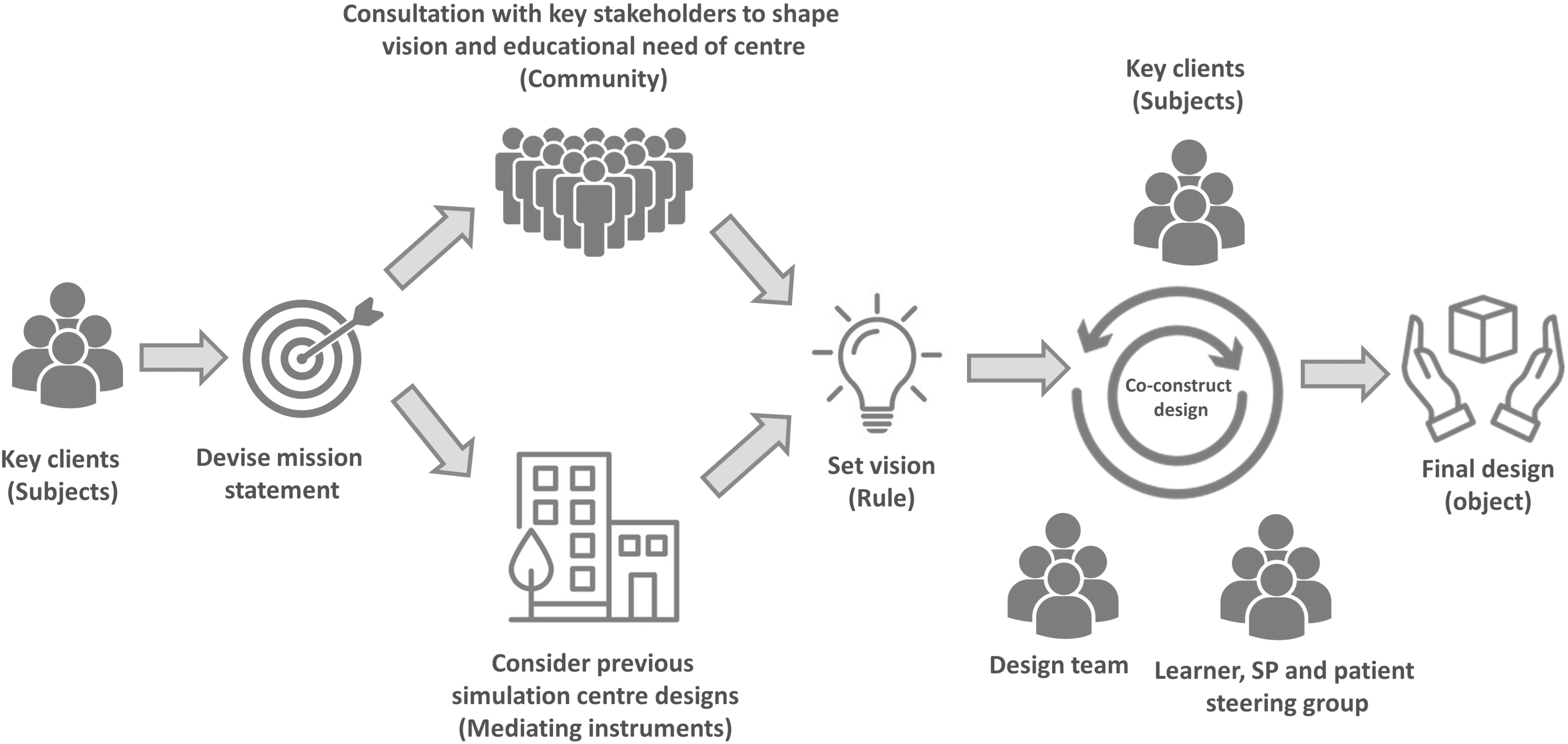
Diagrammatic representation of a simulation centre design process informed by Culture Historical Activity Theory.
Bringing together a diverse group of individuals (subjects) who will manage the project. From the outset, it is important they have a shared understanding of the goal of the centre (object) and not lose sight of its educational objectives. Materializing a mission statement (mediating instruments) can be an important exercise in enhancing the collaboration between the subjects throughout the design process (Figure 6) and ensuring that the education purpose (object) of the centre is not lost in the design process.
Example of a mission statement in the design of a simulation centre.
Having members of your team (division of labour) to engage with key stakeholders (community) to envisage the purpose and future function of the centre is an important step. Visiting other established simulation centres and understanding design features that worked well, or not, can also be useful. These ‘stories’, and indeed images (mediation instruments), will help shape the vision and inform the new simulation centre design. Working with the professional design team through an iterative and dialogic process, thereby reaching a consensus on the requirements of the centre, will result in an informed design process that best serves the needs of the learner, educational faculty, institution and other stakeholders.
Now we will turn our attention to how pedagogical theory can be integrated into the design and physical space of a new simulation centre. To understand how the built environment can support learning, we need to consider how people learn through simulation. Simulation-based education aims to create realities that afford individuals immersive and guided opportunities to develop a range of skills. Such simulated learning realities are particularly relevant to developing high acuity skills – that have few learning opportunities afforded in real clinical environments – such as managing a patient who is having a cardiac arrest or a patient with crisis in their mental health.
Learning via simulation-based education is a complex process, rarely linear and subject to a myriad of influencing factors. Despite this, there are recognized patterns as to how individuals learn in simulated environments. Educational theories offer us insights to these patterns. They help to explain the complex and often variable phenomena of how people learn. There are a wide range of educational theories that guide our understanding of simulated-based teaching and learning. For the purpose of this paper, we will draw upon three social-cultural learning theories, given their importance to the social dimensions of learning that occur in simulation, namely: Community of Practice (CoP) [2], Bakhtinian dialogism [3] and Zone of Proximal Development (ZOP) [4]. During the design process of our new simulation centre, aspects of these theories helped to guide discussions and influenced the final product of our interdisciplinary simulation centre.
Communities of practice (CoP) are formed when individuals engage in a process of collective learning in a shared activity [2]. In simulation centres, learners, faculty and technical staff come together and collectively aim to provide a quality learning experience that will have a positive impact on patient care. The three key elements that constitute a CoP include a ‘domain’, a ‘community’ and ‘to practice’.
First, a CoP is not just a random network of connections between people. The group of people have a group identity defined by a shared domain of interest – i.e. providing a quality learning experience by means of simulation. Membership of this group implies a commitment to the domain. Aside from learners, faculty staff and simulation technicians, simulated participants (SPs) are an important group of professional individuals who make valuable contributions in simulation-based education worldwide. Therefore, it is important by means of the built environment that SPs are encouraged to be part of this learning community and share this domain of interest, in providing the best learning experiences to make a positive impact on patient care. A tangible way of encouraging SPs to be part of this community is to have a dedicated social and functional space for them. Physical objects such as an area for refreshments, soft seating and mirrors can afford practical measures for SPs in the preparation for their roles, applying moulage and de-roling following a simulation learning session. Moreover, having a dedicated space for SPs signals an important commitment to this group of professionals and encourages their input to the community of practice and learning dynamics within the centre (Figure 7).

Simulated participant lounge.
Second, in pursuing their interest in the domain of providing learning by simulation, individuals need to engage in joint activities in this community. They share information with each other, build relationships and assist each other in the activity. They build relationships that enable them to learn from each other, share collective responsibility for providing quality learning experiences and are accountable for their teaching. In the design of our centre, working with SPs and individuals with lived experiences of illness was integral to the process. Being part of this community permitted actual patients and SPs to encourage and challenge the design team, add to and enhance the design of the centre to achieve the best learning experience for our learners. An example of this was to include video spectacles (and the supporting technological infrastructure) that could be placed on high-fidelity manikins, so that the patient’s perspective during a simulation learning activity could be captured. This patient’s video footage can then be used to enhance the patient-centred orientation of the debriefing process (Figure 8).

Video glasses to provide a patient point of view perspective on learner feedback.
Third, a CoP is not just a community of interest. They are practitioners who have a shared practice. They share resources, equipment and experiences to address a particular challenge, in our case enhancing learners’ skills by means of simulation-based education. Therefore, in the design of any simulation centre, the design should enhance individuals to form a community of shared interests and provide a space to optimize interactions and enhance the practice of learning. In the design of InterSim, interprofessional education was recognized as fundamental to the ethos of the centre in helping to develop and train healthcare professionals who recognize the importance of the healthcare team within the real world of clinical practice. Rather than having dedicated zones for each health profession, we intentionally designed simulation spaces that facilitated open, collaborative and interactive forms of pedagogy. These simulation spaces reflected various locations of healthcare in the real world, rather than being discipline-centric. This included a simulated ward, an acute care zone (which could be configured for a number of contexts including a resuscitation room, intensive care unit bay, day procedure unit, general practitioner treatment room, maternity delivery suite), outpatient zone (that could be used as community consultation rooms or hospital outpatient rooms) and a home environment. In order to promote greater inclusiveness in the CoP in the centre, we incorporated a Highly Immersive Virtual Environment (HIVE) zone that can create a wide range of different environments (e.g. specific contexts such as pre-hospital emergency care locations, computerized tomography scan suites, operating theatres, etc.) (Figure 9). This further evidences our commitment to be inclusive in our CoP, where individuals from many disciplines can come together, yielding enhanced resources for our educational practice.

Highly Immersive Virtual Environment (HIVE).
Social interaction, mediated by language and dialogue, is central to learning in simulation-based education. The Russian theorist, Mikhail Bakhtin explicated the notion that meaning comes about through dialogue [3], not just dialogue with others, but with the world around us, our past and future selves. In terms of simulation education, meaning and learning are supported not only by dialogue between students and teachers, but also by students considering their dialogue with other students, and with their previous and future professional selves. Simply conducting a simulation activity will not optimize learner development. Learners need to engage in dialogue that supports their sense-making and in transforming their skills. It follows that supporting opportunities to promote dialogue and ‘learning conversations’ should be crucial to the design of any simulation centre, and not just considered as an afterthought.
One tangible way of promoting learning conversations in a simulation centre is to have dedicated spaces for debriefing sessions. In so doing it not only allows for such learning dialogues, but also communicates the importance placed on debriefing, so much so that it warrants its own dedicated physical space (Figure 10). In addition to the built space, the physical use of furniture can also encourage dialogue and learning conversations. Rather than using standard rectangular desks, plectrum desks can orientate learners to face each other, whilst also viewing a video screen that can be used to play video footage as part of the debriefing process, thereby promoting learners to engage in dialogue and being in a position to also pick up on non-verbal cues from each other.

Learning conversation suite.
Aside from the formal dedicated spaces for debriefing, creating other spaces for conversations can afford important opportunities for learning dialogue. Therefore in the design of our centre we incorporated small booths in the corridors of the simulation centre to allow for ad hoc , spontaneous conversations (Figure 11). For example, after a simulation exercise a learner may hang back, wanting to share their experiences with a faculty member, or alternatively a small group of learners may want to take a short time out to discuss the exercise, whilst they recharge their smartphones. It is clear that these relatively simple physical spaces can afford important and enrichening learning dialogues.
Seating area.
Simulation-based education aims to create a shared space between learner and teacher. Within this safe space, or zone, all strive to create new learning, i.e. ‘learning of something that is not yet there’. This safe space of learning is known as the ZOP. The concept of ZOP was developed by the Russian psychologist Lev Vyogtsky [4]. Vygotsky defines the ZOP as the distance between the actual development level as determined by independent problem-solving and the level of potential development as determined through problem-solving under adult guidance or in collaboration with more capable peers. In Vygotsky’s framing of learning, he considered it to be a participatory process that is mediated by tools and social interactions (e.g. learners developing acute clinical care skills by participating in a simulation with cardiac manikins and teachers debriefing following the scenario). In the supportive relationship between student and teacher, learners aim to expand their skills and ‘go the extra distance’, relative to what might be possible if they were working on their own. From this perspective, simulation-based education is a social endeavour, and one which is embedded in the cultural and physical surroundings of a simulation centre. As typical of most simulation centres, teachers can control a manikin-based simulation from a control room, as they help extend learners from their comfort zone into the supported learning zone.
Extending students beyond their comfort zone can be challenging for them, both psychologically and emotionally. If not supported they can experience intense negative emotions, such as shame and fear [5]. Therefore, in the safe physical environment of a simulation centre we should strive to support learners as they engage in such emotionally charged forms of experiential learning.
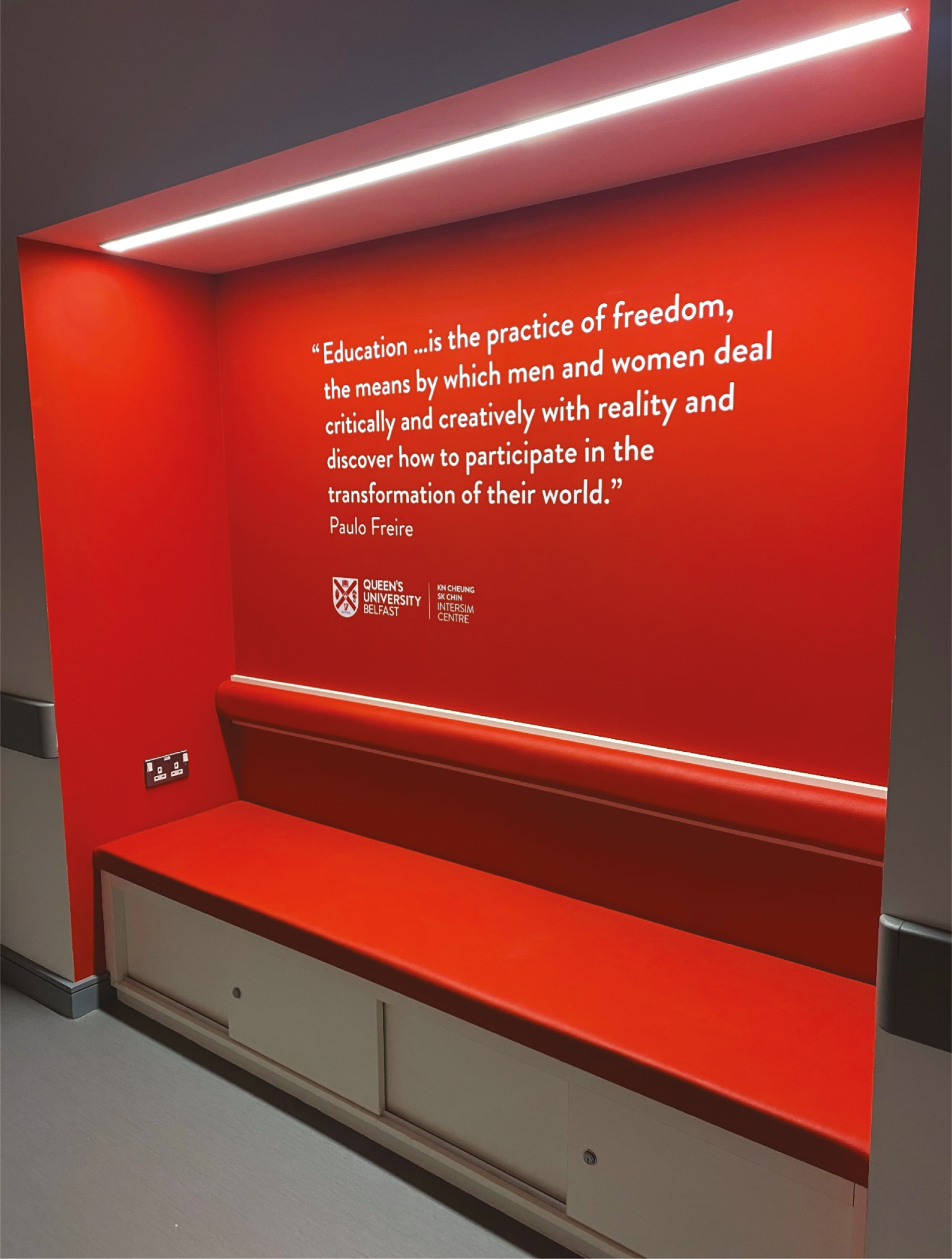
Artefacts, symbols and signs are one physical way of conveying a supportive learning environment in a simulation centre. For example, the reception area of a simulation centre can signal an important first impression to learners as they arrive in the centre. Rather than a stark, sterile waiting area, having an area that conveys a professionalized approach to learning and its commitment to support learners is important. Having some soft seating for learners to wait before they enter the centre, providing water fountains and signs that help to set an appropriate learning culture in the centre can all aid this. The use of signs through the centre can also reinforce the supportive message and positive learning-focused culture of the centre (Figure 12).

Lobby area of InterSim.
The physical spaces in simulation centres have more impact on the effective learning in such environments that one might first imagine. Rather than merely locations to site learning, well-designed and pedagogically informed physical spaces in simulation centres have potential to impactfully enhance the learning process. Moreover, the physical space, objects and symbols within the centre can be ‘carriers of meaning’ that interact with learners as they socially construct their world and promote a learner’s individual agency. In its design, the physical space of a simulation centre brings learners, teachers and facilitators together and should encourage interaction, exploration and reflection during the learning process.
As learners interact with teachers, providing space that promotes the social practice of learning is important in any simulation centre design. With increasing understanding of the underpinning learning theory, never has there been a better time to integrate such learning theory into the design of simulation centres.
Simulation centres can represent one of the most expensive outlays for any healthcare education and training facility. As a simulation community there is a need for us to have a greater understanding of how learning theory can and should be embodied into the design of a simulation centre. Further research into the design of simulation centres can provide more objective evidence of how learning theory can help inform the design decisions of developing simulation centres fit for purpose and the future.
We acknowledge all the members of the InterSim Project Implementation Group in the Faculty of Medicine, Health and Life Sciences, Queen’s University Belfast who have championed and worked together in the design of the new simulation centre at Queen’s University Belfast. We also acknowledge the design team from Ostick and Williams Architects, Belfast, in their invaluable contribution to the centre’s design. We are indebted to the Estates team at Queen’s University Belfast for their professionalism and commitment to the design and build of the centre. Finally, we are indebted to the many generous donors who helped us realize our new InterSim centre.
None declared.
None declared.
Not applicable.
None declared.
None declared.
1.
2.
3.
4.
5.
 Shaping buildings to shape learning: building pedagogical theory into the design of a simulation centre
Shaping buildings to shape learning: building pedagogical theory into the design of a simulation centre
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets