
Our study aimed to examine the communication behaviours of receivers responding to a speaking up message from a nurse. Specifically, what behaviours receivers of the speaking up message used to understand and address their concerns, and whether observed receiver communication behaviours differed between the health disciplines (receiver groups).
Deductive content analysis, through the application of Communication Accommodation Theory, was used to analyse observed receiver behaviour.
We used simulation to directly observe speaking up interactions. Data collection occurred between May and November 2019 within a large metropolitan health organization. Twenty-two simulations were conducted and analysed, involving participants (n = 138) from varying (N = 3) clinical discipline groups.
Nurses/midwives frequently utilized task-based questioning, which inhibited their ability to promptly recognize the speaker’s concern. In contrast, medical officers more readily provided reassurance and support to the speaker and sought clearer understanding of the situation through using more open-ended questioning techniques.
Simulation was an effective means to study receiver behaviour. Results demonstrated the receiver’s clinical discipline influenced not only what behaviour strategies were deployed, but the effectiveness of the strategies in accurately interpreting and effectively resolving the raised concern. This study has important implications for clinical practice and how receivers of a speaking up message are trained. As different disciplines approached the same conversation in very different ways, understanding these differences is key to increasing the efficacy of healthcare speaking up training.
What this study adds
Speaking up is voicing a concern for the prevention of error and/or harm (physical and/or psychological) to healthcare staff and patients [1]. The definition of speaking up appears relatively straightforward, yet the reality for health professionals, it is not so simple. Miscommunication (including a speaker’s inability to speak up or having concerns ignored) is a significant contributor to patient harm [2]. There are a number of well-known barriers to speaking up, including hierarchy and fear of retribution [3] and poor organizational culture [4]. In addition, how a message will be received, including the anticipated response, or lack thereof, is a consistent challenge for clinicians when trying to speak up [5]. What is lacking in the healthcare speaking up literature is an empirical understanding of why receivers of a speaking up message respond as they do. To date, speaking up training tries to theoretically understand the receiver’s response, but little research on speaking has focused on the receiver’s perspective.
Some initial receiver-focused research within speaking up conversations is underway in the perioperative environment. Lemke and colleagues [6] studied the receiver behaviour of anaesthetists during anaesthetic induction, and Long et al. [7] in the general perioperative environment. More recently, theory-driven research, through the application of Communication Accommodation Theory (CAT [8]), has also examined the perceptions of health professional receivers from multiple disciplines and clinical environments (Barlow et al., 2022a). The current study used CAT to examine the behaviour of receivers.
CAT has been widely applied in healthcare communication research. For example, CAT has been used to study open disclosure conversations after medical error [9], nurse–doctor interactions [10], communication between medical specialties [11], and nurse–parent communication [12]. Healthcare is a rich intergroup environment, where salient professional identities can be defined by clinical discipline, seniority level, and clinical specialty or department. As an intergroup theory of communication, CAT is well suited to this environment, as it provides a framework to predict and understand intergroup interactions (e.g. between disciplines or departments) and their associated power differentials [8]. The theory posits that an individual’s communication goals, motivations and drivers of their communication behaviour, are influenced by their salient group identity (the most prominent identity within that interaction) [8]. In previous studies, the authors have demonstrated that speaking up conversations regarding patient care are intergroup interactions, influenced either by a discipline, e.g. nurse being spoken up to by a doctor, or seniority level, e.g. junior nurse being spoken up to by a senior nurse [13].
Social Identity Theory (SIT) explains how individuals within an interaction use behavioural strategies to establish, maintain or make themselves positively distinct from their speech partner, based on group membership [14]. Informed by SIT, CAT theorizes behavioural communication strategies people employ to manage their social relations with others [8]. When using accommodative strategies, similar to therapeutic communication, the person aims to adjust their language and tone to aid comprehension, build empathy and trust and minimize power differentials [12]. In contrast, nonaccommodative behaviour serves to maintain or extend the power differentials and does not facilitate comprehension. Nonaccommodative strategies serve to differentiate a speaker from their conversational partner [8].
Giles [8] explicates that there are five main communication strategies interactants use: approximation, interpretability, discourse management, emotional expression and interpersonal control. Approximation occurs through communication behaviours such as the adjustment of speech patterns, e.g. volume and pitch, rate and tone of speech and non-verbal behaviour to be similar or convergent (accommodative), or dissimilar or divergent (nonaccommodative) to their speech partner. The strategy of Interpretability refers to using language to help (or hinder) comprehension of the message by one’s communication partner. The speaker evaluates their speech partner’s ability to comprehend what they are saying and adjusts (or not) their language (including vocabulary, pronunciation, gestures) accordingly. An example of accommodative interpretability is when a speaker uses language and terminology to aid comprehension. Nonaccommodative interpretability refers to the use of language and jargon unique to a speaker’s health discipline, which may not be readily understood by a conversational partner from another discipline or specialty [10]. The strategy of Discourse Management refers to the interaction process, rather than the content of the conversation. When accommodative, it involves actively engaging the conversational partner, by encouraging participation through manoeuvres such as expanding the content, using open-ended questions and back-channelling, e.g. head nod, or saying mhmm. When nonaccommodative, active engagement from the other person is not encouraged or considered [12]. The strategy of accommodative Emotional Expression concerns appropriately meeting the emotional needs of a conversational partner, by actively acknowledging their needs and providing reassurance. It involves behaviours to ‘save face’, maintain relationships, give reassurance and show concern when appropriate. Emotional expression also includes the speaker regulating their own emotions and emotional expressions (warmth, happiness, appreciation) to maintain the social relationship. Nonaccommodative emotional expression occurs when the emotional needs of the other are ignored or not recognized, and/or a speaker does not regulate their own emotions and expressions to meet the other’s needs. The strategy of nonaccommodative Interpersonal Control refers to a conversational partner’s attempts to constrain a speaker in a specific role through the utilization of power differentials. When a speaker is accommodative, opportunities are created for their speech partner to move outside of their prescribed role [10]. An example of accommodative interpersonal control would be a senior clinician inviting a more junior clinician to voice their opinion (speak up) regarding the care of a patient.
The current study involved direct observation of receiver behaviour during a speaking up situation (discharge planning team) in a defined context using simulated (laboratory) conditions. The study had two research questions. First, what CAT strategies do receivers use to assist their understanding of a speaking up message to address the concerns of the speaker (a nurse)? Second, to investigate if the observed receiver communication behaviours differed across health disciplines (receiver groups).
This study took place in a large Australian tertiary healthcare organization that provided both public and private adult, obstetric and neonatal health services. A purposive sample was sought, as the study required groups of participants from varying clinical disciplines seniority levels, who had protected time to participate in the simulation activities. Participants were recruited from an organizational-wide corporate speaking up training program which used simulation as a standard program activity. The inclusion criteria required that participants be qualified clinicians, who were over the age of 18 years and who voluntarily consented to participate. A minimum sample of 20 participants per receiver group (nursing/midwifery, allied health, medical officers) was targeted, to achieve sufficient data for a medium-sized qualitative project [15] that would provide a unique insight into each receiver group.
One hundred and thirty-eight clinicians participated in the simulations. They consisted of nurses/midwives (n = 96), allied health, comprising of social workers, physiotherapists, radiographers, pharmacists and phlebotomists (n = 22), and medical officers (doctors) (n = 20). Most participants were from inpatient wards (n = 48) and critical care areas (n = 26). Years of experience ranged from being a new graduate or intern with less than 3 years’ experience (n = 44), through to more than 20 years of clinical experience (n = 15). See Table 1.

| Characteristic | Nurse/midwife | Allied health | Medical officer | |||
|---|---|---|---|---|---|---|
| N | % | n | % | n | % | |
| 96 | 69.5 | 22 | 16.0 | 20 | 14.5 | |
| Clinical specialty | ||||||
| Critical care | 18 | 18.8 | 1 | 4.5 | 7 | 35 |
| Perioperative | 13 | 13.5 | 0 | 0 | 2 | 10 |
| Inpatient wards | 35 | 36.5 | 8 | 36.4 | 5 | 25 |
| Day stay areas | 1 | 1.0 | 0 | 0 | 0 | 0 |
| Antenatal areas | 2 | 2.1 | 3 | 13.6 | 0 | 0 |
| Birth suite | 7 | 7.3 | 0 | 0 | 2 | 10 |
| Outpatients | 4 | 4.2 | 4 | 18.2 | 2 | 10 |
| Interventional areas | 5 | 5.2 | 3 | 13.6 | 0 | 0 |
| Other | 8 | 8.3 | 2 | 9.1 | 2 | 10 |
| Missing | 3 | 3.1 | 1 | 4.5 | 0 | 0 |
| Years in profession | ||||||
| 3 years or less | 29 | 30.2 | 5 | 22.7 | 10 | 50 |
| 4–8 years | 22 | 22.9 | 7 | 31.8 | 2 | 10 |
| 9–14 years | 11 | 11.5 | 4 | 18.2 | 5 | 25 |
| 15–20 years | 7 | 7.3 | 3 | 13.6 | 1 | 5 |
| More than 20 years | 11 | 11.5 | 2 | 9.1 | 2 | 10 |
| Missing | 16 | 16.7 | 1 | 4.5 | 0 | 0 |
| Gender | ||||||
| Male | 11 | 11.5 | 6 | 27.3 | 10 | 50 |
| Female | 85 | 88.5 | 16 | 72.7 | 10 | 50 |
Allied health: social work, physiotherapy, radiography, pharmacy and phlebotomy
All participants received a standard e-mail reminding them of their attendance to the corporate speaking up training program, which included the Participant Information and Consent Form (PICF). Participants arrived with either their completed consent form or had an opportunity at the start of the training program to ask the lead investigator any questions regarding the activity and their involvement. Participants could choose to consent (or not) up until the commencement of the simulation activity. Participation in the research did not impact participants meeting the requirements for successful program completion. Participants self-enrolled into the speaking up program; therefore, it was unknown to the research team on any given day what clinical disciplines would be present and who would consent to participate. As a result, each simulation differed in group size and clinical discipline representation. Of the 22 simulations, at least two nurses/midwives were present in each simulation, medical officers were present in 11 and allied health in 10 simulations.
Within the simulation, participants were the discharge team, and upon entering the patient’s room, the junior bedside nurse, Mary (embedded simulated person), spoke up about her concern for the patient (manikin voiced by a simulation technician) going home without the appropriate and required home care in place. The pre-booked ambulance was on the way to transport the patient home, which contributed to a time pressure regarding decision-making. Owing to the need to get a timely decision, Mary had asked for her patient to be reviewed first by the discharge team, but her patient was, in fact, the last patient to be reviewed. The bedside nurse in all simulations spoke up using ‘hint and hope’, a commonly cited methodology used by nurses [16]. The two different speaking up messages were alternated across the 22 simulations. Both were accommodative but delivered with differing degrees of accommodation. One message was delivered by the nurse in a very polite manner, giving a lot of information (verbose), but not directly stating (instead hinting) the main concern. Alternatively, it was delivered in a less accommodating, less polite manner, which was more succinct and abrupt, and still did not clearly articulate the main concern (see Table 2 for examples). There was no clear nonaccommodative speaking up message, as it was deemed unrealistic that a more junior nurse, when faced with speaking up to a multidisciplinary team, would be openly confrontational. To investigate communication dynamics, the speaking up message was delivered to the team, rather than to a specific individual. Who responded, and how that response was framed, was completely up to the receivers.
| What Mary was thinking | What Mary actually said |
|---|---|
| The patient lives alone with no home support. She is a high falls risk. Mary is thinking the patient should not go home today due to high risk of falling. The ambulance transport needs to be cancelled and a comprehensive discharge plan organized. |
Message 1: Hint and hope – Accommodative, verbose Thank goodness, you’re here. This is Mrs Williams she’s due to go home today. The ambulance is coming within two hours, but the discharge has not been organized. So, I’m really worried that the appropriate care is not going to be in place. I really think we need a decision like now, whether she can go home or not. As I said, the discharge is not in place, so wondering what your thoughts are. |
| Message 2: Hint and hope – Less accommodative, succinct/abrupt Look, I asked the ward receptionist if you could start the ward round here, not finish here. I’ve got the ambulance transport coming to pick up Mrs Williams and none of the discharge has been done and I don’t think she’s ready to go home. So, I just need you to do something. |
After the simulations, participants undertook a structured debrief, as reported elsewhere [17]. The simulations were designed and delivered according to international standards in simulation and by educators trained in simulation methodology [18].
All simulations were video recorded by both Go-Pro camera and the simulation centre’s inbuilt audio-visual (AV) system, to mitigate the risk of AV recording failure. Data were collected between May to November 2019. All 22 simulation videos were reviewed for audio quality, and all were included for analysis. The simulations were transcribed verbatim using NVivo transcription software (Version 12) [19] and cross-checked by the lead author against the video recordings.
This study had Human Research Ethics Committee and Research Governance approval from the health organization HREC/18/MHS/78 and received ethical clearance from the university.
During the transcription process all identifiable participant data from the simulation activity were removed. All demographic data were analysed using descriptive statistics in SPSS (Version 28) [20]. To analyse the simulations we used a deductive qualitative content analysis approach [21]. This analysis approach aimed to extend current knowledge on speaking up, by observing receiver behaviour in action and aligning their communication behaviour to CAT strategies. The codes for analysis were predetermined according to CAT behaviour strategies: approximation, discourse management, emotional expression, interpersonal control and interpretability. Receiver behaviours, as appropriate, were then assigned to a CAT strategy. All receiver responses within each speaking up encounter were eligible for analysis, regardless if it was one individual who responded as the receiver, or multiple receivers. In a single receiver response, if the participant implemented different behaviours, more than one strategy was coded to that response.
To achieve data immersion, the lead author (MB, nurse) read the transcripts at least three times prior to coding. An initial coding sheet was then drafted for the first round of coding to identify accommodative and nonaccommodative communication behaviour examples for each CAT strategy. These examples were developed from the current speaking up literature, which suggests what receiver communication behaviour can occur. The lead author then completed three rounds of coding, checking in with a CAT expert each time to clarify interpretation and understanding of CAT strategies. With each round of coding, receiver behaviours within the coding sheet were refined. Data were also coded against the video recordings to align participant non-verbal behaviour and speech patterns against the transcript.
A second coder from a different clinical background (psychology) and an expert in CAT (BW) then independently coded 50% of the transcripts using the final version of the coding sheet. The differing clinical specialties of the coders helped to ensure analysis of the data was viewed from different lens, rather than through a nursing-centric lens. Reflexive notes were taken throughout the process, and the meetings between coders to reach consensus were recorded. See Appendix A for the coding sheet. The interclass correlation coefficient (ICC) for absolute agreement to ascertain interrater reliability was calculated for the 50% double-coded data, using mean-ranking, two-way mixed effects model [22]. There was a high degree of reliability between the two raters on the 11 double-coded simulations. The average ICC was 0.931, with a 95% confidence interval from 0.873 to 0.962. This study followed COREQ guidelines for qualitative analysis.
Twenty-two simulations were run, recorded and analysed. The simulations ran for a mean of 4.52 minutes (range 3.0–7.24 minutes), SD 1.06. A total of 264 codes were identified from all receiver responses.
During the coding process, the coders (BW, MB) agreed that it was difficult to clearly analyse what aspects of receiver behaviour aligned to the strategies of discourse management and approximation. This difficulty arose because several receivers within an interaction asked short and direct questions, which meant it was not possible to accurately gauge approximation. For example, there was no opportunity to map how much receivers matched the speaker’s tone of voice. For discourse management, video angles did not always allow the receiver’s faces to be clearly visible. This meant that analysis of the receiver’s facial expressions or gestures that might signal encouragement for the speaker to continue the conversation was not able to be consistently analysed. As the interactions represented technical conversations, where obtaining relevant information was paramount, the strategy of interpretability was identified as the primary strategy rather than discourse management. When the receivers sought further clarification of the concern, it was apparent that they were not encouraging the speaker’s engagement in the conversational process, but rather required additional important information to help their interpretability of the concern. For these reasons the strategies of approximation and discourse management were removed from analysis. A key tenet of CAT is the influence of context. Where and when the conversation is occurring is theorized to influence the strategies individuals deploy. Therefore, it is not unexpected that receivers in our study used some strategies more than others. The three remaining CAT strategies of interpretability, interpersonal control and emotional expression were analysed by comparing the use of the communication strategies between the three receiver groups (nursing/midwifery, allied health, medical officers) and across speaker message types (accommodative/verbose, less accommodative/abrupt).
Across receiver groups, most receivers displayed accommodative behaviour (nonaccommodative behaviours n = 2) regardless of which of the two messages were being delivered. To compare the frequency of accommodative CAT strategies used per receiver group, the rate of codes for each CAT strategy was calculated as a proportion of the sample size for that receiver group (see Figure 1).

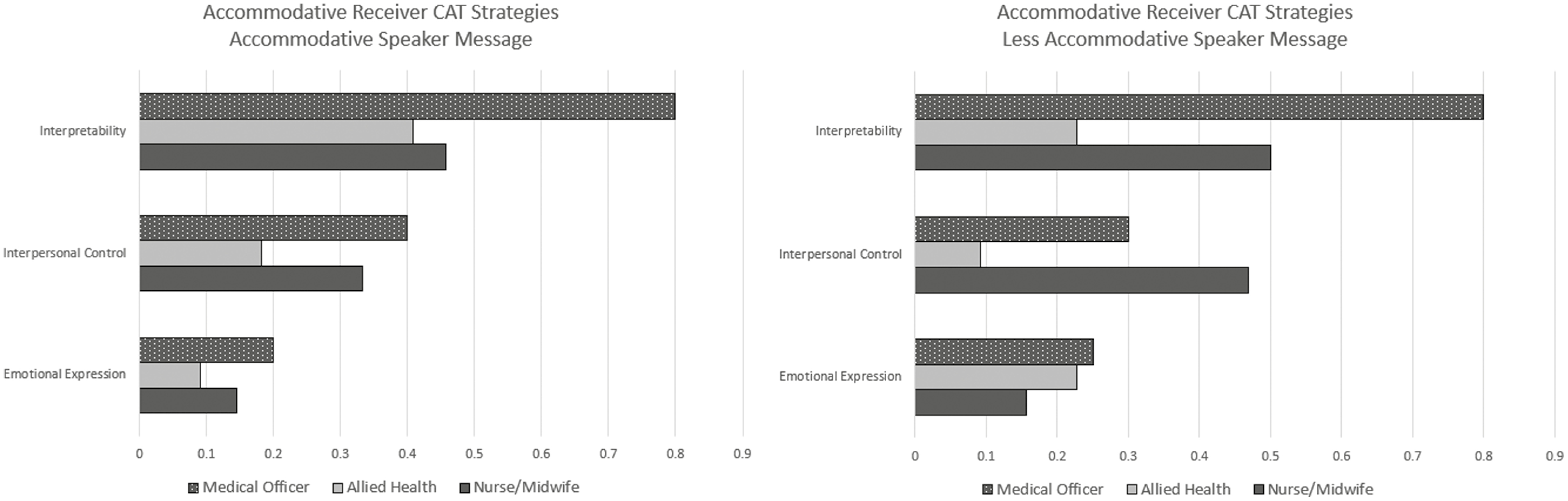
Number of codes per CAT category in relation to sample size per receiver group
The receiver seeking further information to gain better understanding of the speaker’s concern was the most frequently coded behaviour across all receiver groups. How these questions were posed, however, differed between receiver groups. Across all receiver groups, the questions asked and the use of paraphrasing to check comprehension of the concern were all evaluated as accommodative. Receivers appeared to genuinely try to accommodate to the speaker’s communication comprehension. When differences occurred, it was in the effectiveness of the questioning approach used to understand and address the voiced concern.
For nurses/midwives, the use of the interpretability strategy did not differ according to the speaker’s behaviour (see Figure 1). Receivers within this group overwhelmingly demonstrated ineffective interpretability by posing questions that aimed to ascertain tasks to be done, to quickly get the patient ready for the ambulance, rather than understand that the patient needed to stay in hospital, as it was unsafe for her to go home, e.g. What are the specific things that we need to get done? What would we need? What needs to be done to get her ready to go? (NM35). This task-based questioning by nurses/midwives in one simulation ensued for 2:56 minutes, before the questioning technique was changed by another receiver group. This task-based questioning was inefficient in understanding the concern and reaching a resolution. For example,
Effective interpretability was demonstrated by some nurse/midwife receivers after receiving the initial speaking up message, by acknowledging that the message had been heard and checking understanding. For example,
We can hear you concerns Mary. And I think, well are you potentially thinking that maybe Mrs Williams isn’t ready for discharge today and we have to rethink the plan? Well, maybe we need to talk about the things that need to happen and whether it’s realistic that can happen today and whether Mrs Williams can go home. (NM59)
Allied health receivers sought greater message clarity through interpretability strategies, more so when the speaker was more accommodative. There were occasions where allied health receivers did display inappropriate interpretability through task-based questioning. These questions were usually focused on their own clinical area of expertise and were often asked before any clarifying questioning occurred. For example, after Mary initially spoke up, a phlebotomist asked as the first receiver ‘Have the morning bloods been done?’ (AH01). One pharmacist asked, ‘Has the discharge been organised, like scripts?’ (AH13).
Appropriate interpretability was demonstrated by several allied health receivers (n = 14) when they focused on comprehending the main concern regarding patient safety, e.g. ‘So, she’s going home, so that is a bit of a red flag moment for me if she’s not going to be safe’ (AH18).
Medical officers’ use of the interpretability strategy was not affected by speaker behaviour (see Figure 1). Of the 11 simulations where medical officers were present, this receiver group was the first to respond to the speaker’s concern (first receiver) on only four occasions. Medical officers tended to stay back and listen to the conversation. It appeared when the questioning by the other receiver groups failed to clearly interpret the concern (up to 2:56 minutes in the conversation), medical officers then stepped forward and sought deeper clarification. Overall, this receiver group’s questioning was not task-focused, rather they sought clearer understanding of the situation through using more open-ended questions, e.g. ‘I hear you say that she isn’t ready for discharge. What do you mean by that?’ (MO17) and ‘can I ask you as you’ve been looking after her all night, can I ask if you’ve got any specific concerns that you want us to address in terms of discharge planning?’ (MO16). In the first example by MO17, this questioning was very effective, as it led to a prompt understanding of the concern, enabling a clear resolution to be reached and the simulation concluding within 2:30 minutes.
Appropriate emotional expression strategies were displayed through using empathy and the provision of reassurance to the speaker. All strategies deployed were verbal. There were no occurrences where any receivers demonstrated non-verbal reassurance, such as the use of touch.
This receiver group deployed the same level of emotional expression strategies regardless of how the message was delivered. Overall, nurse/midwife receivers demonstrated less emotional expression than other receiver group (see Figure 1). This receiver group did not often openly acknowledge the speaker’s emotions or provide direct verbal reassurance. When it was demonstrated, the receiver thanked Mary for speaking up ‘So, thank you for your concern. Sorry, you’re under a lot of pressure’ (NM23). One receiver (NM08) demonstrated appropriate emotional expression by validating Mary’s clinical ability in identifying the safety priority and providing ingroup empathy regarding clinical workload.
So, I think I can hear what your concerns are Mary. And it seems like you’ve done a really good job of seeing what the patient’s priorities are. And I think you’re stressed because you’ve had a huge shift in discharging all these patients. (NM08)
Allied health receivers demonstrated more emotional expression strategies when the speaker was less accommodative. They did this by either acknowledging the speaker’s emotions and/or empathizing with the speaker’s situation, e.g. ‘Well, Mary, I can say that you are quite stressed and a lot of pressure on your plate to get Mrs. Williams home’ (AH02), and ‘it sounds to me that you’ve had a lot of pressure and you wanted to do it right, you know. And that’s what we all want. We all want what’s best for Mrs Williams’ (AH06).
Allied health receivers also paired emotional expression and interpretability together ‘Mary, that’s a reasonable concern. Do you know how Mrs. Williams is mobilising right now?’ (AH18), and ‘I hear that you are feeling frustrated about the situation. Yeah, I’m thinking that maybe we need to have some more discussions to see what your concerns are’ (AH06). This pairing provided the speaker with validation of their concern, and then sought further information to enhance understanding of the situation.
This receiver group were the most frequent demonstrators of appropriate emotional expression strategies across all receiver groups (Figure 1) and displayed more emotional expression when the speaker was less accommodative. Medical officers most frequently thanked the speaker and acknowledged the act of speaking up; ‘I’m glad you brought it up. So, I think it’s a very big point where she’s come in with a fall there is no point sending her home if it’s going to happen again. So, I think that’s really worthwhile’ (MO17), and ‘Those concerns are all very valuable and important, thank you for sharing them’ (MO08).
Medical officer receivers also demonstrated more strategies that attempted to build rapport with the speaker, through introducing themselves and acknowledging the speaker’s frustration of the delayed review by the discharge team ‘Mary, [receiver’s name] is my name and I don’t think we’ve met before. I’m one of the doctors. I’m sorry first of all for taking so long to see you. I think we weren’t aware that you were waiting for us’ (MO03).
Appropriate interpersonal control behaviours were demonstrated through empowering the speaker to share their thoughts and opinions, and by promoting equality (reducing hierarchy) between the junior nurse speaker and the receiver group. Again, most receivers displayed appropriate interpersonal control strategies, with only two occasions of inappropriate (nonaccommodative) interpersonal control demonstrated across all simulations.
Nurses/midwives demonstrated more use of interpersonal control strategies when the speaker was less accommodative. For the nurse/midwife group, appropriate interpersonal control was demonstrated by asking Mary the nurse for her opinion and thoughts, and for her active participation in the process ‘So what are your plans Mary? What would you like to see happen? (NM63). It was also demonstrated by the receiver bringing the speaker in as part of the team, and decision-making process.
I’m thinking that maybe that is something that we really need to discuss as a team and work with you (speaking to patient), and you Mary (nurse), to really plan this discharge thoroughly. And I’m wondering, what you need from us and what we can do as a team? (NM26)
During the interactions where nurses/midwives were using inappropriate task-based questioning, one nurse/midwife stepped forward as the receiver and took control of the situation to have the team pause and give themselves time to think of a way forward, ‘Well, I think we just need to take a minute and not rush this whole thing. What are you thinking guys?’ (NM57).
Often appropriate interpersonal control strategies were used in combination with appropriate emotional expression behaviours. In the below example, the receiver provided emotional support to the speaker, attempted to build rapport through introducing themselves, and then appropriately took control by stating a plan of action.
That’s a really tough decision. But thank you very much for voicing your opinion on the matter. We are sorry that it did take a while for us to get around to you. Let me first introduce myself, so I’m [name]. It’s really lovely to meet you, Mary. We might just say hello to the patient first. And what we’ll do from there is to discuss with our team and see if we could call the after-hours coordinator and see if she can advise us on it. (NM28)
Comparatively, allied health receivers demonstrated less interpersonal control behaviours than other receiver groups (Figure 1), particularly when the speaker was less accommodating. When allied health receivers used accommodative interpersonal control, it was in a decision-making process, ‘Let’s speak to the team leader about the ED [emergency department] patient. Because I don’t think it is safe to send her home when she has no family support and no discharge planning done’ (AH14).
Allied health was the only group to demonstrate nonaccommodative interpersonal control on two separate occasions. Both occurred in simulations where the speaker was less accommodating. The first was where the allied health receiver bluntly and unilaterally stating a decision.
The second occurrence was evaluated as nonaccommodative due to the tone of voice in which it was said, as it came across as accusatory, ‘So why is she being discharged if there is no one to help her?!’ (AH20).
Unlike nurses/midwives, this receiver group displayed more appropriate interpersonal control strategies with the more accommodating speaker, to move the conversation forward to a resolution, e.g. ‘I just don’t think that this woman is fit for discharge today, I think she needs to stay tonight until we get her sorted’ (MO17). Some receivers were successful by pairing appropriate interpersonal control with emotional expression strategies; validating the speaker’s concerns, and appropriately taking control of the situation for required decision-making.
Thank you for bringing this to our attention. If you’re concerned, we are all going to be concerned. I think we put patient safety first, which is very appropriate and I support that, I think she’s needs to stay in hospital. (MO05)
The aim of the study was to investigate what CAT strategies receivers used to assist their understanding of a speaking up message and how receiver behaviour differed between health disciplines and across the two message types. Speaking up messages were delivered using the hint and hope methodology in either an accommodative, or less accommodative manner. How the speaking up message was delivered made some subtle observable differences in the receiver’s behaviour, particularly in the strategies of interpersonal control and emotional expression. Certainly, all receiver groups overwhelmingly displayed accommodative communication behaviours towards the speaker. Accommodative behaviours reflecting CAT strategies have been demonstrated to reduce the social distance between groups and thereby enhance communication outcomes [23]. However, the extent to which receivers accommodated towards the speaker and the CAT strategies they used, differed between the clinical disciplines. Additionally, the complexity of speaking up interactions was highlighted by receivers often using a combination of CAT strategies in their response.
Combining CAT strategies was a shared behaviour across all receiver groups, which appeared to both enhance the receiver’s understanding of the concern and meet the speaker’s needs. The use of emotional expression with either interpretability and/or interpersonal control were the most utilized by receivers. Uncertainty about the correct interpretation of the concern, fear of being wrong and/or fear of retribution are well-documented barriers to speaking up for clinicians [24]. The deployment of accommodative emotional expression by receivers (e.g. validating the speaker’s concern, demonstrating gratitude by thanking the speaker for speaking up, and demonstrating empathy) was important in building rapport, reducing the associated fear of speaking up and enhancing speaker engagement in the conversation. Once clarity of the concern was gained, receivers appropriately took control to move the conversation forward. Receivers often did this through offering suggestions and seeking consensus with the team and speaker.
Receiver identity (clinical discipline) influenced receiver behaviour. Interestingly, nurses/midwives demonstrated more interpersonal control when the speaker spoke in a less accommodative manner than an accommodative one. Within the debrief, this receiver group evaluated the less accommodative speaker as being frustrated and stressed. Attempting to take control of the situation was therefore deployed as a supportive measure for their ingroup member (nurse speaker). It was unexpected that nurses/midwives overall displayed the least emotional expression behaviours, given they are typically viewed as ‘the caring profession/s’ [25]. This behaviour was explored in the debriefs, where ‘listening to fix’ was identified as the largest barrier to effective receivership [17]. Nurses/midwives stated that ‘fixing’ the problem was their way of demonstrating emotional support to the speaker. The problem with this behaviour is two-fold. Firstly, we know from the literature that speaking up is hard, particularly for those in lower hierarchical disciplines [3]. Therefore, receiver support and emotional expression behaviours need to be explicit, rather than implicit to encourage participation in both the immediate and future speaking up interactions. Secondly, by asking task-based, ‘fixing’ questions, identification and understanding of the concern was delayed. If this behaviour was adopted in clinical situations where patient harm was imminent, this could potentially have dire consequences [2].
Regardless of the level of accommodation, the indirect nature of the messages (hint and hope) influenced interpretability of the concern. This forced receivers to implement strategies, often unsuccessfully, to try and achieve clarity. Speaking up mnemonics aim to help the speaker voice a succinct and clear concern [26]. There is, however, extensive research demonstrating that despite mnemonics and training, speaking up remains difficult, particularly in the presence of power status differentials between the speaker and receiver [27]. Like the junior nurse speaker in this study, the vague, hint and hope methodology is widespread amongst nurses, particularly when speaking to medical officers [16], and has also been noted in speaking up conversations during anaesthetic induction [6]. From our findings, it seems crucial that receivers are trained to receive a message. Receivers need to know how to manage self in the moment, to get curious and question further and to use open-ended questions that seek to understand, rather than to fix.
When observing allied health behaviour across the two message types, more emotional expression and fewer interpretability strategies were observed in the less accommodative simulations. This finding could reflect that when the speaker is less accommodating, allied health shift their behaviour from questioning to the provision of emotional support. This finding does align with our previous work, where more than any other receiver group, allied health was able to make positive attributions (accommodating emotional expression) about a nonaccommodative speaker [28]. The making of positive attributions, e.g. the speaker is concerned for patient safety, increased their perceptions of the acceptability of the message.
Medical officers were influenced the least by the speaker’s communication behaviour. This supports previous findings [29] where this receiver group evaluated both accommodative and nonaccommodative messages as equally acceptable [29]. It was expected that doctors would step forward as the first receiver, given their hierarchical positioning in the multidisciplinary team; however, this did not occur. Instead, medical officers stood back, listened and stepped into the conversation when a resolution was not readily forthcoming, which proved a successful tactic. The delayed engagement in the conversation may have been influenced by differences in communication training and role expectations between the disciplines. Clearly, how a message was heard and responded to, differed according to clinical discipline, and may account for why current speaking up training and standardized mnemonics are not always successful [30].
Regardless of discipline, it often took some time in the simulation for participants to realize they were being spoken up to. Participants were briefed prior to the simulated encounter; however, they were intentionally not informed as to whether they were going to be the speaker or receiver within the interaction. We acknowledge that delays in recognition and deployment of appropriate behaviour adjustments may have been influenced by the simulated context. Currently speaking up programs routinely only rehearse the act of speaking up and not receiving [31], which we believe is a key contributing factor. We argue that this lack of recognition or awareness of being spoken up to due to vague messaging readily occurs in real clinical practice. Receivers, therefore, may be being judged as ignoring the speaker and their concern, which may in part account for reports of inadequate receiver behaviour within the speaking up literature.
A key strength to this study was the application of a robust communication theory to analyse directly observed receiver behaviours. CAT highlighted how different disciplines have different approaches to receiving the same information. This finding has not previously been explicitly noted in the literature, and sheds light on an additional reason why speaking up remains difficult despite standardized mnemonics. Understanding differences between disciplines is important to increasing the efficacy of healthcare communication training.
There were limitations to the study. The speaker in all the simulations was a nurse. Whilst this allowed a consistent comparison of receiver behaviour, it needs to be noted that receiver behaviour may have been different if the message was delivered by another discipline. It must also be noted that for some clinicians, being a member of a patient discharge team was not part of their normal clinical role and may have affected their ability to engage. We do argue though that you do not have be a content expert to effectively listen and help facilitate a curious conversation. Participants knew they were being watched, and the fact that the clinical situation was not an emergency, high-stress, or high cognitive load event may have contributed to the accommodative stance of nearly all receivers. The literature from the speaker’s perspective has often reported poor or nonaccommodative receiver behaviour [32]. This requires further investigation. The situation however did allow for the elicitation and observation of unique communication behaviours by different receiver groups. To further enhance transferability, future studies should use CAT to observe receiver behaviour in high-stakes situations, where patient harm is imminent.
We compared the pattern of behaviour between receiver groups by the receiver being part of a group of clinicians who were the ‘discharge team’. This was a strength of the study, but also a limitation, as it meant that the strategies of approximation and discourse management could not be identified for individual receivers. Future studies should use CAT to observe and examine the speaking up interaction between a speaker and a single receiver. In addition, this study highlights the complexity of isolating communication strategies that may co-occur.
This study has important implications for clinical practice and how receivers of the message are trained. Based on the results of the study, training clinicians to be receivers of a speaking up message needs to be an explicit component within speaking up training programs. The use of CAT strategies has been shown to be helpful in training clinicians to effectively manage patient aggression [23]. From the results of our study, we believe that it could also provide a framework to equip clinicians with a range of strategies to implement as receivers of a speaking up message.
From the findings, it appears that nurses/midwives may need to learn how to listen more effectively to a message. This includes how to position themselves to be willing to focus not only on the tasks to be completed, but also to investigate what is it that the speaker is trying to convey. This requires teaching clinicians how to listen to understand, rather than to fix, and that listening is not a passive activity; rather, it requires a willingness to engage [33] and to manage one’s own emotional reactions [4]. To effectively interpret the speaking up message requires deliberate moves by the receiver, including giving oneself permission to pause [13] and to be curious. Emotional expression serves to enhance speaker engagement and should be a standard element of the response. Receivers would do well to thank and acknowledge the speaker for speaking up. Note, this does not mean the receiver has to agree with the concern; rather, it is a step to build rapport and mutual respect, to allow further exploration of the concern and to navigate a way forward [4]. In addition, the receiver needs to learn how to appropriately utilize the strategy of interpersonal control, by recapping or paraphrasing to check understanding, suggest options with a rationale and to seek consensus. By training the receiver in these strategies, speaking up conversations become less reliant on remembering speaking up rubrics/mnemonics, and instead shifts the focus to seeking understanding, shared negotiation and achieving a shared resolution.
Speaking up is important for patient safety and effective clinical care; however, little is known about how people respond to speaking up messages. We found clinicians used the strategies of interpretability, emotional expression and interpersonal control to receive and respond to the speaking up message. How these strategies were deployed differed between the three discipline groups and with varying degrees of effectiveness in meeting the speaker’s needs. The findings have direct application to speaking up training for both speakers and receivers and demonstrate CAT could be used to help frame and inform recommended receiver strategies to enhance speaking up communication within and between disciplines. Clinicians being trained to respond effectively to speaking up messages will both improve patient outcomes and enhance the occurrence of clinicians voicing their concerns.
The authors would like to acknowledge Kate Morse, Fiona Maccallum and Robert Simon for their intellectual contributions to the design of this study and the clinicians who participated.
MB is the primary author and undertook this work as part of a PhD, at University of Queensland. BW and EJ contributed to methods, data analysis and critical review of the manuscript.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The data that support the study findings are available from the corresponding first author, upon reasonable request.
This study had Human Research Ethics Committee and Research Governance approval from the health organisation HREC/18/MHS/78 and received ethical clearance from the university.
The authors report there are no competing interests to declare.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
Coding for CAT strategies and exemplars for receiver behaviour
| CAT strategy | Explanation | Coding criteria | Exemplars |
|---|---|---|---|
| Interpretability | Receivers adjust their language to ensure they are understood by speaker. Receiver response seeks clarification if the message is not understood |
-Verbally acknowledge they have received and understood the message, e.g. stating ‘I understand’, ‘I hear you’, or repeating back what has been said to them -Actively seeks clarification of the speaker’s concerns if required to ensure understanding -Receiver repeats the concern raised to verify that they have understood the message -Receiver use standard terminology and unambiguous language during the speaking up conversation -Pays attention to speaker’s non-verbal language to see if speaker has understood receiver’s message, e.g. nods head or, non-understanding. |
‘So, Mary, your concerned and I think it’s not clinically safe for Mrs Williams to go home today. So, I think we need to address those issues’ (NM42). ‘Mary, I’m hearing that you sound like you think it’s unsafe for Mrs. Williams to go home. Is that what you’re saying?’ (NM35). ‘I hear you say that she isn’t ready for discharge. What do you mean by that?’ (MO17). |
| Emotional expression | Receiver provides reassurance to the speaker and demonstrates empathy to help meet speaker’s emotional needs. | -Receiver expresses gratitude for speaking up, says ‘thank you’, and acts in a manner that encourages ongoing vigilance -Acknowledges and empathizes how speaking up can be difficult and anxiety provoking -Is openly receptive to the speaker’s thoughts/perspectives -Speaks/responds from a stance of curiosity, does not make assumptions about speaker’s intent -Receiver notices speaker’s anxiety or frustration, verbally acknowledges and provides reassurance through touch or language, e.g. places hand on arm. |
‘Thank you for bringing this to our attention. If you’re concerned, we are all going to be concerned. I think we put patient safety first, which is very appropriate and I support that’ (MO05). ‘[Let’s] discuss what is best for Mrs. Williams because it sounds to me that you’ve had a lot of pressure and you wanted to do it right, you know, Mary’s wanting to do the right thing by you, Mrs. Williams. And that’s what we all want’ (AH06). ‘So, thank you for your concern. Sorry, you’re under a lot of pressure’ (NM23). |
| Interpersonal control | Receiver acknowledges the speaker’s concerns regardless of rank, status, discipline. | -Receiver pays attention to where positioned in relation to speaker (not standing over). -Does not interrupt or ignore the person speaking up -Receiver appropriately takes control of the situation to help move the conversation forward -Receiver respectfully shares their agreement/disagreement and rationale with the speaker -Receiver tries to find a mutually acceptable resolution and checks back in with speaker after agreed intervention/way forward completed -Differences in perspectives are focused on the topic (what), not the person (who) -Acknowledges speaker speaking up and recognising that the person speaking up can feel intimidated, e.g. encourages speaker to share their concerns and rationales, thanks the speaker for their efforts/bravery, invites input (sharing concerns) from others in the team. |
‘I’m sorry Mary, can I just escalate this further. So, I’m concerned as Mrs. Williams is hearing all the concerns and I think these are nursing concerns from now on and probably a bit [sic] logistical concerns. It doesn’t involve Mrs Williams anymore. Do you mind if we talk somewhere else?’ (NM30). ‘So maybe we should step out, have a look at the chart. Just make sure the boxes are ticked or we initiate the right people being involved. And then we can regroup and make sure that the plans in place. and everybody is happy. Does that sound okay? I know it will take a little bit more time now, but it means we’ll have a really good safe plan in place and hopefully keep you home rather than be here in hospital.’ NM68 ‘I just don’t think that this woman is fit for discharge today, I think she needs to stay tonight until we get her sorted’ (MO17). |
| Approximation | Did not analyse | ||
| Discourse management | Did not analyse |
 Understanding observed receiver strategies in the healthcare speaking up context
Understanding observed receiver strategies in the healthcare speaking up context
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets