The nursing team is crucial in emergency care (EC) settings, serving as patients’ first point of contact. However, gaps in their training have been hindering the effectiveness of care and patient survival. In situ simulation (ISS) has been recognized as a valuable tool in EC education, uncovering hidden risks in clinical care areas. This study aimed to analyse how an ISS educational intervention in the EC department impacted participants’ clinical and transferable skills.
To assess the effectiveness of an educational intervention on the 37 EC nursing professionals, a 12-month study quasi-experimental study was conducted. The study consisted of a survey to identify participants’ learning needs and four workshops tailored to meet the team’s specific needs, culminating in an ISS session. Knowledge levels were evaluated using pre- and post-tests administered before (T0) and after (T1) the workshops, along with a formative assessment with an Objective Structured Clinical Examination (OSCE) holistic marking guide to measure the clinical and transferable skills acquired during the ISS.
The primary participant’s learning needs centred around cardiopulmonary arrest caused by acute myocardial infarction, including interpreting electrocardiogram and teamwork. These topics were used to develop the workshop and the simulation scenario. A significant difference (p < 0.001) was observed in the levels of learning between T0 and T1, indicating a marked improvement in the participants’ performance. The nursing professionals displayed proficient clinical and transferable skills during the ISS, successfully completing over 80% of the OSCE items.
These findings suggested that a customized educational intervention incorporating participatory learning and ISS effectively enhances clinical and transferable skills among nursing professionals. The positive outcomes observed in post-tests and OSCE holistic assessment highlighted the effectiveness of this intervention for the EC nursing team. The results of this study demonstrate that active participation in workshops facilitates knowledge acquisition. Furthermore, the OSCE results illustrate the practical application of clinical and transferable skills during the ISS.
What this study adds
In emergency departments, the nursing team plays a pivotal role at the forefront of the service, serving as the initial point of contact for patients. Their significance in upholding the standard of emergency care (EC) cannot be overstated. Therefore, the team must keep updated training in appropriate competencies and skills to manage critical care clients [1,2]. However, gaps in the training have been considered obstacles in EC [2,3] since the effectiveness of care is proportional to the patient’s survival [4]. EC education promotes knowledge and skills to recognize and manage life-threatening symptoms [5,6].
In situ simulation (ISS) has been acknowledged as an important part of training in EC to uncover latent threats in clinical care areas. ISS is a team-based training technique conducted in the actual patient care environment using equipment and resources from that unit and involving actual healthcare team members [7]. The educational value of ISS is the principles of learning tied to the context of the experience [8] and the participatory experience based on patient care and the reality of the health unit itself [9–12] without great costs to the institution [10,13].
ISS recreates critical stressful events that require complex skills application, such as decision-making and team interaction in a safe environment [9,10,13]. Other advantages of ISS are (a) reinforcement of concepts about high-risk health situations, (b) development of clinical skills and performance, (c) identification of possible system failures and (d) patient safety [9–11,13]. However, limited information about the effects of ISS integrated into an educational intervention is available, highlighting this research’s importance. This study aimed to analyse how an ISS educational intervention in the EC department impacted participants’ clinical and transferable skills.
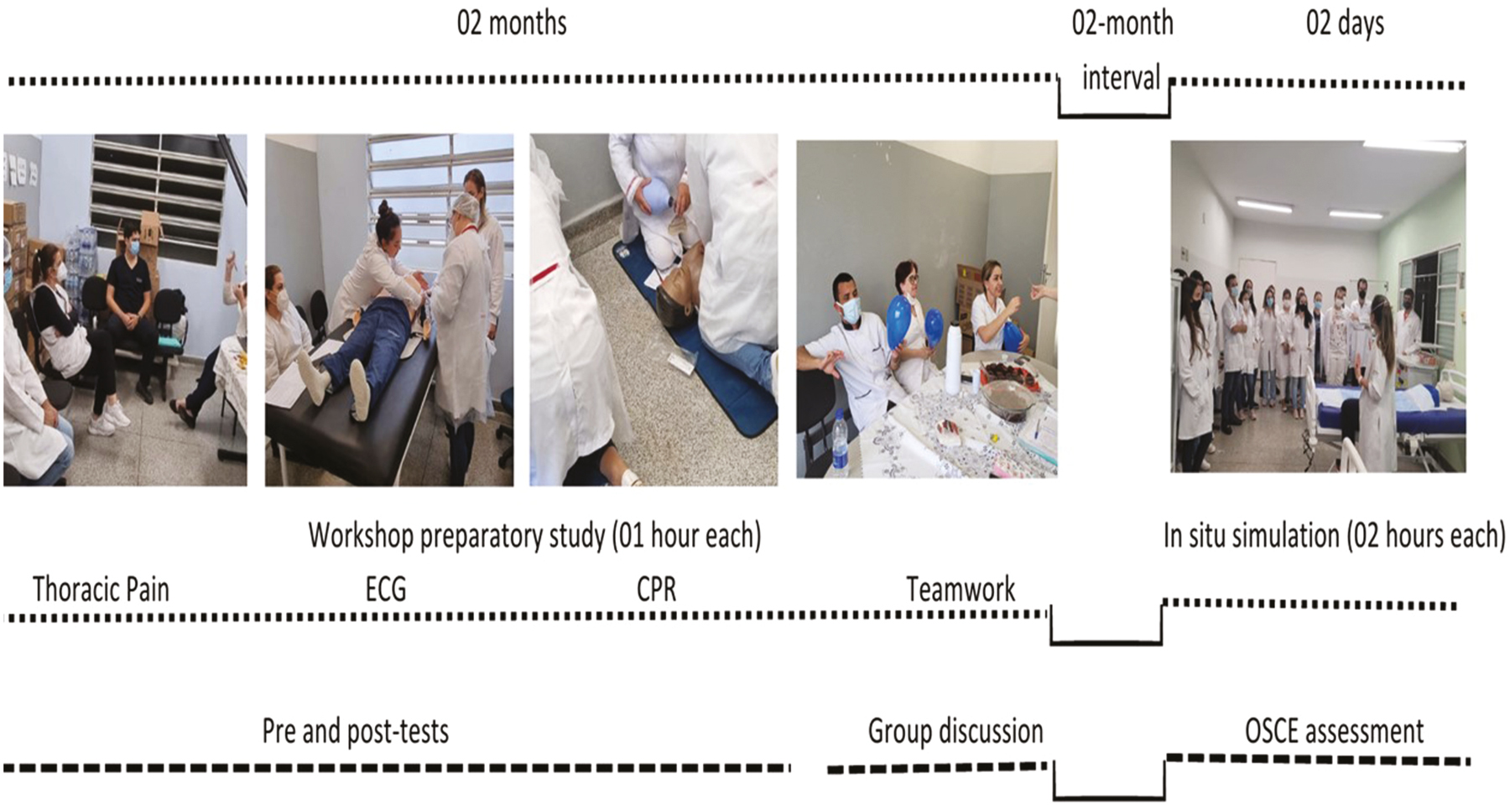
A quasi-experimental to evaluate an ISS educational intervention [14]. The knowledge was measured with a one-group pre-test–post-test design by questionnaires before (T0) and after (T1) the workshops (see details in the Instruments section). After completing the workshops, a formative assessment using an Objective Structured Clinical Examination (OSCE) holistic marking guide was used to assess clinical and transferable skills applied by the participants during the ISS (Figure 1). The study took place at an Emergency Department in the countryside of Sao Paulo state, Brazil. It was approved by the local ethics committee (protocol number CAEE 31526420.2.0000.5393).

Study design
In August 2020, 12 registered nurses and 25 practical nurses were invited to participate in the study at the healthcare unit. All nursing professionals (37) agreed to participate by giving their informed written consent, and none were excluded. The ISS educational intervention was offered as optional for their required professional development hours. They participated in four workshops and one ISS, grouped into eight teams of 6 to 3 members based on their rotation schedule. For each rotation, two groups were formed to guarantee the continuation of care.
The ISS educational intervention included workshops and the ISS. During the second semester of 2020, the participants answered a socio-demographic questionnaire and a survey to identify their learning needs based on their work routine at the health unit. They ranked their major learning needs from 1 to 10, including cognitive, procedural and attitudinal learning. The selected topics varied from clinical to transferable skills, including (a) patients with thoracic pain, (b) electrocardiogram (ECG), (c) cardiopulmonary resuscitation (CPR) care and (d) teamwork. These topics were used to develop the four workshops and the case study for the ISS. Although there is a need for more consensus in the literature [15], clinical skills are understood to encompass practical procedures, assessment, diagnostic and treatment/therapeutic skills and communication [15]. Transferable skills refer to the ability to apply something learned in one context to another, such as communication, teamwork and problem-solving [16], which is particularly important in nursing.
The participant’s knowledge was measured in two moments: (1) by comparing pre- and post-test results immediately before (T0) and after (T1) the workshops; (2) the clinical and transferable skills were measured through expertise observation using the OSCE holistic marking guide during the ISS. A nursing research team and experts from the Clinical Simulation Learning Center at the University of São Paulo at Ribeirão Preto College of Nursing delivered the ISS educational intervention.
Four workshops took place between April and May of 2021 to prepare the participants for the ISS. Before workshops a, b and c began, the participants were offered the session purpose and the pre-test (T0). They participated in active learning related to the topic and their work routine at the unit. Each activity used a discussion of previous learning, a brief lecture, hands-on training and a group discussion. Ultimately, they filled out the post-test (T1) for each session. Then, the corrected answers were provided by the principal investigator. Pre- and post-tests were applied in workshops a, b and c. For the workshop d – teamwork, a group discussion of their experiences was used to replace pre- and post-tests. The discussion was used to support the ISS case study.
In August 2021, each nursing professional was assigned to a team to participate in the ISS. The goal was to provide an additional formative learning opportunity for the participants to apply clinical and transferable skills in a controlled and safe learning environment. Skilled facilitators conducted one ISS for each team, including pre-briefing, CPR role-play with a standardized patient and debriefing. The dose of the simulation was the same for each participant. For each session, nurses worked through the CPR case, taking into account the aggregation of their previous learning developed in the workshops (see Supplementary Appendix 1). The case study designed for the ISS included: objectives, a description of the scenario (i.e. facilities to create the required perception of realism), a situation and backstory, clinical progression, cues for the advancement of the case, performance measures and critical actions for the nursing team [10]. The ISS sessions were recorded and delivered in an unused emergency room in the healthcare unit. The clinical case and the simulation session definitions are included in the online supplement (see Supplementary Appendix 1). An OSCE holistic marking guide was embedded in the ISS due to participant’s time restraints; two skilled nurses worked individually, observing the participants throughout the ISS and manually completing the marking guide.
The survey gathered data on respondents’ gender, age, years since graduation and tenure at the healthcare institution. The type of socio-demographic questions and options offered to participants followed the Research Ethics Board recommendations.
The questionnaire about learning needs was developed based on the most frequent nursing care in the unit. It was organized into a diagnostic hypothesis (understood here as the cognitive aspects of learning), procedural, attitudinal/managerial care (Supplementary Appendix 2). To construct the questionnaire, the principal investigator carried out a 10-hour non-participant observation to identify the nursing activities carried out in the unit. Three experts in urgency and emergency were invited to assess the clarity of the questionnaire’s content, with 100% agreement and approval of the content clarity.
The 10 questions used in the workshop “a” were developed by the researchers and evaluated for content and appearance by five experts in the field, with 100% agreement and approval in content clarity (Supplementary Appendix 3). The questions used in workshops b and c were not evaluated, as they were open-access, validated questions available online for training purposes (five questions each).
The OSCE holistic marking guide assessed participants’ clinical and transferable skills performance during the ISS [17,18] due to limited participant availability for a separate, dedicated OSCE activity. It adhered to the best practice OSCE guidelines [17] to develop a Likert scale (correct, partial, incorrect and not performed) with 25 items as follows: (a) 12 questions already validated [18] and (b) the development of 13 questions about cognitive and attitudinal learning to contemplate the themes addressed in the workshops. These 13 questions were evaluated by five experts in EC and clinical simulation with 100% agreement and approval on the clarity of content. Furthermore, the holistic marking guide was employed to facilitate group discussions and elicit participant feedback regarding their performance during the debriefing session.
The data from the socio-demographic questions, the learning needs questionnaire, the pre- and post-tests and the OSCE were manually entered into Microsoft Excel. As said previously, two skilled nurses independently fill out the OSCE for each ISS; for one ISS, a third nurse was assigned to review the recorded session due to disparities discovered during the comparative analysis.
Descriptive statistics were used to analyse the participants’ sociodemographic data and learning needs. Paired-sample t-tests were used to determine whether the participants gained more knowledge after workshops a, b and c. Descriptive statistical analyses were applied to analyse the OSCE data. The analysis was processed in the IBM® SPSS®, version 25, adopting the significance level α = 0.05.
Among all participants, 15 identified themselves as male and 22 as female. Most of them completed the nursing program more than 10 years ago (21, 58.2%). Of the total, 11 (30.5%) worked at the healthcare institution for less than 5 years.
The primary learning needs for nursing professionals centred around team performance in the care of cardiopulmonary arrest (CRP) (37/37) caused by acute myocardial infarction (AMI) (32/37), including ECG (37/37) and teamwork (28/37).
In each workshop, the participants completed a pre- and post-test about the (a) patients with thoracic pain, (b) ECG and (c) CPR. At least 25 individuals (69.4%, teamwork) to 31 individuals (86.1%, ECG) completed the series of four workshops and pre- and post-tests. Upon comparing the performance of participants before and after attending all the workshops, the Wilcoxon test revealed a significant difference (p < 0.001) in the levels of learning (Table 1).

| Workshops | Pre-test | Post-test | p* value | ||
|---|---|---|---|---|---|
| Mean | Mean (%) | Mean | Mean (%) | ||
| 1 – Thoracic pain (10 questions) | 6 | 60 | 8.7 | 87 | <0.001 |
| 2 – ECG interpretation (05 questions) | 2.5 | 50 | 4.5 | 90 | <0.001 |
| 3 – CPR care (05 questions) | 2.3 | 46 | 4.5 | 90 | <0.001 |
Of 37, 25 (69.4%) nursing professionals completed the ISS successfully. They demonstrated accurate clinical and transferable skills to perform over 80% of the OSCE items. Only question 23 was partially achieved by 33.3% of the participants, while 66.7% still needed to attempt it (Table 2).
| OSCE items | Correct | Partial | Incorrect | Not performed |
|---|---|---|---|---|
| 1. Welcomed the patient based on humanized care | 12 (100%) | |||
| 2. Checked signs and symptoms presented by the patient | 10 (83.3%) | 2 (16.7%) | ||
| 3. Associated the signs and symptoms with vital signs | 10 (83.3%) | 2 (16.7%) | ||
| 4. Questioned the patient about chest pain: location, irradiation, duration and associated factors | 12 (100%) | |||
| 5. Questioned the patient about risk factors: morbidities, smoking and heart disease | 10 (83.3%) | 2 (16.7%) | ||
| 6. Considered the possibility of an acute myocardial infarction, based on the clinical evaluation | 8 (66.7%) | 4 (33.3%) | ||
| 7. The patient’s complaints were heard and considered | 12 (100%) | |||
| 8. Considered the severity of the patient and the possibility of CPR | 8 (66.7%) | 4 (33.3%) | ||
| 9. Requested help from the health team | 10 (83.3%) | 2 (16.7%) | ||
| 10. Used clear communication with the patient | 12 (100%) | |||
| 11. Used clear communication with the health team | 10 (83.3%) | 2 (16.7%) | ||
| 12. Was able to work as a team | 10 (83.3%) | 2 (16.7%) | ||
| 13. Shared tasks with other colleagues to ensure the quality of the care | 12 (100%) | |||
| 14. Ensured scene safety for patient care | 12 (100%) | |||
| 15. Used personal protective equipment | 8 (66.7%) | 4 (33.3%) | ||
| 16. Played intensely at the patient’s shoulder level with intense auditory stimulus to confirm unresponsiveness | 8 (66.7%) | 2 (16.7%) | 2 (16.7%) | |
| 17. Assessed patient’s pulse and respiration simultaneously | 6 (50%) | 4 (33.3%) | 2 (16.7%) | |
| 18. Positioned the patient on the bed with the headboard at 0°, without a pillow and with a shield (board) to start external chest compression (ECC) | 6 (50%) | 6 (50%) | ||
| 19. Upon the absence of patient pulse and breathing: Positioned themself parallel to the patient’s chest, on the auxiliary ladder, with arms and legs stretched out, legs apart, hands overlapping, hypothenar region of the hand on the patient’s sternum, fingers interlaced, shoulder at the level of the patient’s chest and movements carried out by the lumbar spine to start the (ECC) | 8 (66.7%) | 4 (33.3%) | ||
| 20. ECC was performed in the lower half of the sternum | 12 (100%) | |||
| 21. ECC was performed with a depth of at least 5 cm but not more than six | 12 (100%) | |||
| 22. Performed 100 but not more than 120 ECC per minute | 8 (83.3%) | 2 (16.7%) | ||
| 23. Elevated patient head with neck hyperextension for upper airway clearance | 4 (33.3%) | 8 (66.7%) | ||
| 24. Attached a mask to the patient’s face with the index finger pressing it and the other fingers pulling the mandible without escaping air (Technique C and E) | 6 (50%) | 5 (41.7%) | 1 (8.3%) | |
| 25. Performed a 30 × 2 cycle – with correct ECC, ventilation and mask positioning | 8 (66.7%) | 1 (8.3%) | 3 (25%) |
This research aimed to understand how an ISS educational intervention impacted the emergency department nursing team. We developed a 12-month-long study with four workshops and an ISS based on the EC nursing team’s needs.
This study was grounded in the perspective that collective educational actions hold greater significance for healthcare professionals, positioning them as active community members [19] and possibly increasing their self-confidence, knowledge and proficiency in carrying out professional practices [20,21]. The nursing team engaged in the discourse surrounding the educational proposal and its subsequent implementation, employing a dynamic and participatory approach [19]. In response to the health team’s learning needs and addressing existing training gaps, this process enhanced professional performance and an improvement in the quality of patient care [20].
The findings of this research offer novel and valuable insights that can inform the development of innovative proposals. The innovative training intervention proposed in this study comprises multiple components, including four workshops conducted periodically to address participants’ learning needs. The evaluation of knowledge construction was facilitated through pre- and post-tests and group discussions. Furthermore, ISS involving the same teams functioning in their work environment was employed alongside an OSCE holistic marking guide to formative assess participants’ performance. Notably, existing literature needs studies with a similar methodology, necessitating a discussion of the results based on related research.
The primary learning need identified in the survey pertains to team-based care for patients experiencing cardiorespiratory arrest. Despite cardiac arrest care being a common occurrence in emergency departments, the survey results align with existing literature, underscoring the challenges and deficiencies encountered by the team in recognizing and effectively responding to the needs of patients [22]. The acquisition of knowledge by the nursing team through professional training is deemed essential to enhance the quality of care and improve patient survival rates [9]. ISS is recommended for cardiorespiratory arrest care as a safe and effective strategy for enhancing professional practice performance [9,23].
During the learning analysis phase, the findings revealed a significant improvement in participants’ performance, as evidenced by a notable difference between pre- and post-test results across all three workshops (p < 0.001). In Workshop 1, it was observed that the participants already possessed a solid understanding of patient reception and management for individuals presenting with chest pain, as indicated by the relatively smaller variation in correct answers between the pre- and post-tests [24]. The acquisition of electrocardiogram knowledge (Workshop 2) demonstrated proficient utilization by the participants and emerged as a critical skill for the unit. Given that the execution of electrocardiogram tracings falls within the purview of the nursing team and is considered the gold standard for diagnosing cardiac arrhythmias, this knowledge acquisition is of paramount importance [25,26]. When a nursing professional is competent to respond appropriately upon encountering an abnormal tracing, the likelihood of providing prompt and effective care to the patient increases, thereby minimizing potential harm [1,25].
The comparison of pre- and post-test results in Workshop 3 indicated that participants encountered challenges in accurately describing the appropriate anatomical site for chest compressions. However, during the practical activity conducted within the workshop, participants demonstrated competence in performing compressions at the recommended location despite their inability to articulate it verbally. Notably, while only one participant answered this question correctly in the pre-test, a significant improvement was observed in the post-test, with 19 individuals providing the correct response.
The literature confirms the results about the effectiveness of educational intervention proposals. An educational intervention focusing on CPR was designed for 113 nursing professionals at EC. Various active teaching and learning strategies were implemented, including flipped classrooms, video lectures, skills training and clinical simulations. Pre- and post-tests measured the intervention’s effectiveness. The analysis of the average percentage of correct responses between the pre- and post-test indicated a significant improvement in knowledge scores (p < 0.001) concerning cognitive competence [27]. This positive outcome may be attributed to effective teaching and learning strategies throughout the educational activity. A similar study assessed the impact of an educational intervention on attitudes towards CPR among healthcare professionals from diverse disciplines within two hospitals. The results revealed a significant improvement in 10 out of 11 items, indicating positive changes in various aspects of CPR-related attitudes [28]. These findings underscore the positive influence of education on shaping healthcare professionals’ attitudes towards resuscitation.
The literature presents similar results regarding using simulation. A systematic review [29] found that simulation-based education positively influenced nursing students’ knowledge, skills and clinical reasoning abilities. Another meta-analysis [30] demonstrated that simulation-based training significantly positively affected clinical competence and self-confidence. Notably, none of the studies in the literature associated active teaching methodologies with pre- and post-test and OSCE assessments.
In this study, we opted to embed a formative assessment in the ISS using an OSCE holistic marking guide. The guide also provided an opportunity to trigger questions to connect their ISS experience performance with real clinical practice during the debriefing [14].
OSCE encourages the integration of theoretical knowledge into practical applications, promoting critical thinking, problem-solving and decision-making abilities [31,32]. A mixed method study [14] evidenced the applicability of the OSCE best practice guidelines to inform the development and delivery of simulation activities in nursing. This assessment approach has emerged as an effective tool for nursing education, allowing for the comprehensive assessment of clinical skills. The standard OSCE approach provides a structured, standardized summative assessment, incorporating multiple stations that simulate real-world clinical scenarios. In contrast, formative OSCEs have been highlighted in the literature as an educational tool, adopting the structure of a summative assessment to offer constructive feedback to learners [33], including EC training programs [34]. In nursing, a formative OSCE assessment poses superior context and meaning during the debriefing compared with a checklist format.
Our study results confirm that training programs using active teaching methods have positive and lasting effects even after completion. It is vital to sustain these interventions and uphold high levels of professional performance in patient care. This highlights the significance of ongoing educational initiatives to maintain and improve nursing skills in clinical practice [35,36].
Factors outside the study are pointed out as this study’s limitations. First, the participant’s rotation schedule made it difficult for the team to participate and enroll in a control group. Second, routine care in the health unit (emergency department) in the 2 months between the workshops and ISS might have influenced participants’ learning and impacted the scores observed during the ISS.
Finally, given the time constraints of the participants, conducting a separate third training session exclusively dedicated to the summative OSCE was not feasible.
Our research suggests that a customized educational intervention utilizing participatory learning and ISS enhances clinical and transferable skills among nursing professionals. The positive outcomes observed in post-tests and OSCE highlight the effectiveness of this intervention.
The results of this study demonstrate that active participation in workshops facilitates immediate knowledge acquisition. Furthermore, the OSCE results illustrate the practical application of clinical and transferable skills during the ISS.
Employing the OSCE holistic marking guide in a formative way not only validated participants’ performance but also stimulated discussion during the debriefing. Gaining practical experience in a controlled and secure learning environment may enhance their self-confidence. A couple of future research is recommended to strengthen the validity of these findings. First, conducting longitudinal studies to evaluate clinical and transferable skills development in participants and their practical application within an EC unit could provide valuable insights for in-depth exploration. Additionally, exploring the applicability of the model used in this study in interprofessional education would be beneficial. Furthermore, researching real patient interactions post-completion of educational interventions could contribute to cultivating a culture of ongoing education.
Supplementary data are available at The International Journal of Healthcare Simulation online.
VBF is the primary author and undertook this work as part of a Master’s Degree at the University of Sao Paulo. FdosSNdeG was the study supervisor. ER and RAAdeC contributed to methods, data analysis and critical review of the manuscript. BFT contributed to the methods and critical review of the manuscript.
Coordination for the Improvement of Higher Education Personnel – Brazil (CAPES) – Financing Code 001.
None declared.
None declared.
The authors declare no conflict of interest.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.

 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets