
Work attributed to School of Obstetrics and Gynaecology, NIMDTA, Belfast.
Gynaecological surgical skills training has changed significantly in recent decades with a move to competency-based frameworks within obstetrics and gynaecology (O+G) and a focus on acquisition of knowledge and non-technical skills [1]. The laparoscopic approach has become the gold standard for many gynaecological procedures since the 1970s [2]; however, training in laparoscopic surgery relies on trainee’s exposure to the operating theatre with a shallow learning curve [3]. Laparoscopic simulation has been shown to steepen this learning curve with the potential to improve patient safety [2,3]. Laparoscopic simulation training is not a replacement for live operating but an adjunct in preparation for clinical practice [3].
Many factors have impacted O+G trainee’s exposure to training in laparoscopic surgery and there has been international concern regarding this [2]. This includes the introduction of the European Working Time Directive, which saw an end to the traditional ‘apprenticeship model’ of training. More recently, the COVID-19 pandemic has significantly decreased operating theatre exposure up to 50% internationally [4]. As part of the gynaecological surgical recovery plan, the RCOG advised that simulation training should be prioritized both regionally and nationally[5]. The aim of this programme was to provide bespoke gynaecological laparoscopic simulation training to all O+G trainees in Northern Ireland (NI) in the challenging post-COVID era.
A survey was sent to all O+G trainees in NI to capture data on trainees’ opinions of gynaecological surgical training following the COVID-19 pandemic. There was an 89% response rate showing that 86% of trainees felt their skills were not appropriate for their training grade and 76% felt they would not be competent in gynaecological surgery at the completion of their training.
In NI, O+G training is provided across seven training units within all five NI health and social care trusts. There are approximately 70 O+G trainees in NI who historically had to travel to a central location for training, which was deemed most accessible for the majority of trainees. Following a discussion at the deanery school board meeting, an expression of interest was sent to all training units in NI to become a member of the laparoscopic simulation team. This dedicated team of simulation leads included a consultant gynaecological champion as well as a trainee simulation lead in every training unit, making up seven laparoscopic simulation hubs across all of NI. Laparoscopic simulation boxes and equipment were distributed to every training hub, depending on trainee numbers within the unit.
A regional laparoscopic simulation curriculum was developed and distributed to all trainees in NI. The curriculum highlighted the effectiveness of laparoscopic simulation within gynaecological training and was broken down into basic, intermediate, and advanced laparoscopic skills. This was linked to the RCOG training matrix for O+G trainees, with images showing how to perform the skills. Table 1 highlights the laparoscopic simulation skills included in the curriculum. The curriculum also included a simulation logbook for trainees to document simulated skills with space for self-feedback and consultant feedback, further simulating the live theatre environment as well as giving trainees the opportunity to provide evidence of simulated laparoscopic skills for their training portfolio.

| Laparoscopic curriculum | Learning objective |
|---|---|
| Basic laparoscopic skills | |
| Thread transfer | Instrument handling, depth perception and dexterity |
| Paper clips untangle | Fine motor skills, problem solving |
| Specimen retrieval | Ambidexterity, fine instrument control |
| Bead stack | Ambidexterity, fine instrument control |
| Intermediate laparoscopic skills | |
| Cyst dissection | Fine instrument control, tissue handling, cutting, simulate laparoscopic ovarian cystectomy |
| Cube stacking | Ambidexterity, fine instrument control |
| Suture threading | Laparoscopic needle mounting |
| Salpingectomy/salpingostomy model | Fine tissue control, simulate laparoscopic management of ectopic pregnancy |
| Advanced laparoscopic skills | |
| Intracorporeal suture and tie | Laparoscopic suturing and tying skills |
| Horizontal suture | Simulate closing the vaginal vault |
| Roeder knot tying | Develop Roeder knot tying technique |
The laparoscopic simulation sessions were held locally in each simulation hub starting with a teaching session, provided virtually, by a consultant gynaecologist with an interest in laparoscopic surgery. This was followed by dedicated time on laparoscopic simulation boxes under the supervision of the simulation leads. This gave the trainee the opportunity to have laparoscopic surgical training, under consultant supervision, within their own training unit. The simulation logbook was then completed, including feedback. This process simulated all aspects of the live operating environment and provided evidence of the trainee’s surgical training in an era of significant reduction in access to theatre and live operating.
A post-course questionnaire was sent to all trainees in NI with responses from every simulation hub and training grade. This included a self-reported score, from 0 to 10, for basic (p ≤ 0.01), intermediate (p ≤ 0.01), and advanced (p = 0.02) laparoscopic skills before and after the simulation programme (Figure 1). All trainees felt that the programme was beneficial to their training and that laparoscopic simulation training should be introduced as a regular component of the regional deanery teaching within O+G.

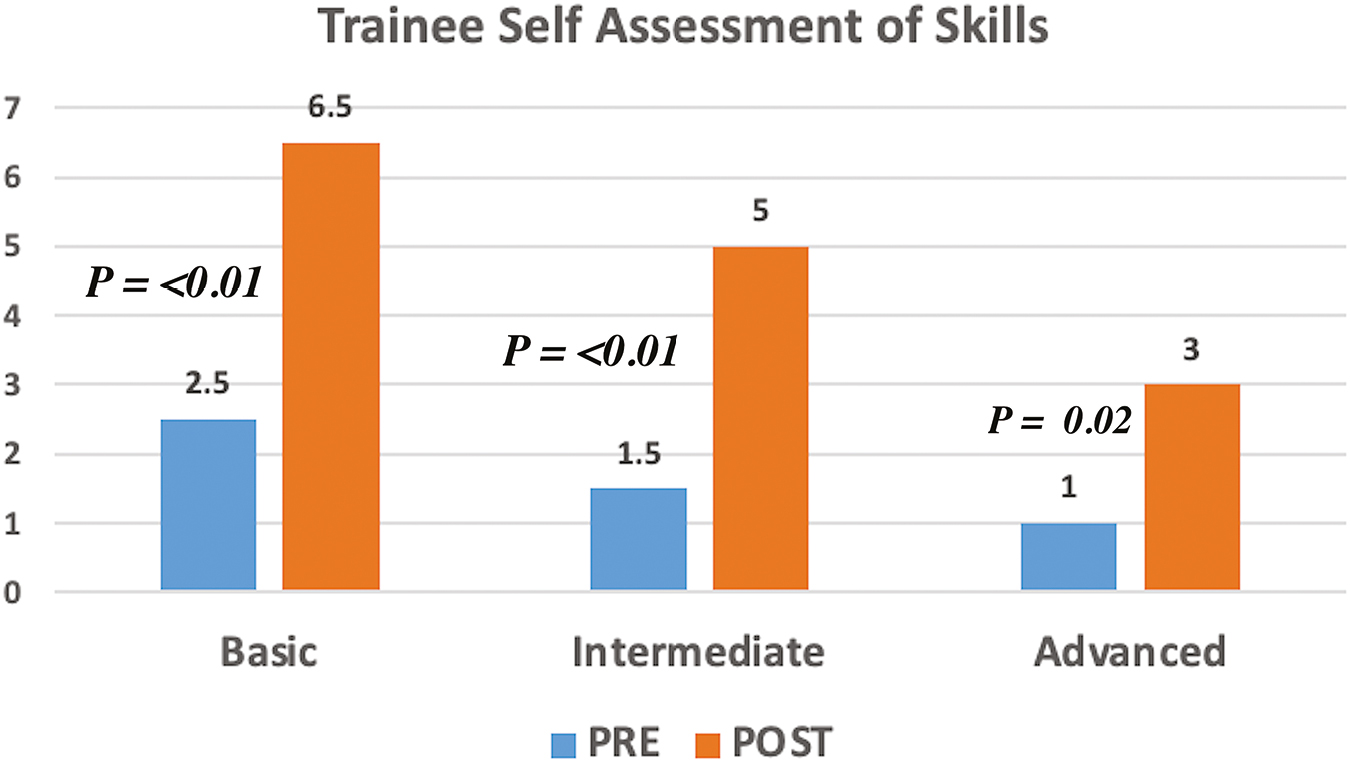
Trainee’s self-assessment of laparoscopic skills before and after the laparoscopic simulation programme. Statistical analysis was performed using Students’ paired t-test.
A regional gynaecological laparoscopic simulation programme was successfully delivered in every O+G training unit within NI, with all training grades reporting a statistically significant improvement in their self-reported laparoscopic simulation skills. Following the success of the programme and trainee feedback, regional laparoscopic training is now provided on a monthly basis, to all O+G trainees in NI, as a regular component of deanery teaching. This laparoscopic simulation training model has also been adopted by other surgical specialties to improve laparoscopic surgical training overall.
JCM: conceptualization, development of curriculum, survey development and distribution, manuscript development. CM, CB: conceptualization, development of curriculum, survey development and distribution, manuscript review. MMcC: conceptualization, development of curriculum, survey development and distribution, manuscript review, supervision.
Northern Ireland Medical & Dental Training Agency (NIMDTA) for funding the purchase of laparoscopic simulation equipment and supporting the access to virtual teaching platforms.
None declared.
None declared.
None declared.
1.
2.
3.
4.
5.

 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets