Elective laparotomies are common approaches to abdominal surgery, providing junior surgeons with opportunities to open and close the abdominal wall cavity under close supervision [1]. Many complications arising from these surgical interventions take place during the surgeon’s initial skills acquisition phase [2]. Simulation-based education (SBE) can facilitate skills development out of the operating theatre through repetitive practice in a safe environment such as a simulation laboratory (lab).
Undoubtedly, practicing these techniques on specimens such as cadaveric and animal tissue remain the most homogenous to human abdominal wall closures. Simulated models described in the literature utilizing porcine tissue, lack full representation of all human abdominal tissue layers and incur operational challenges in tissue acquisition and disposal due to restrictive policies associated with biological tissue [3]. Other simulator modalities and the general cost of SBE programmes can be prohibitive, requiring consumables, human resources and logistics [2].
The aim of this report is to introduce an impactful, replicable, low-cost abdominal wall incisional and closure training model as a pilot, with true anatomical representation as a learning tool for junior surgical trainees.
The model development team comprised collaborative expertise between healthcare simulation technicians, healthcare simulation educators and a consultant surgeon in this domain of practice. Using principles of functional fidelity [4], the spiral model [5] guided the evolutionary design and fabrication process, which included model refinements with expert surgical input.
A prototype training model was developed based on anatomical specifications from collaborating surgeons to simulate a midline abdominal incision and closure. One simulation technician (AFR) took written notes on the detailed feedback obtained throughout the review and evaluation phase, which were later entered on to a Microsoft (MS) Excel™ spreadsheet. Based on this expert feedback, simulation technicians brainstormed suggested design improvements. These suggestions were coded in traffic light format, with those in green or amber categories considered for application to the next iteration of model development. Suggestions in the red category were deemed unsuitable after careful analysis.
Once suggested improvements were made to the model, the development and testing phase would be repeated again, with a consultant surgeon (JMO’R) carrying out all the tasks on the model that it was designed to simulate. The surgeon gave feedback on the model’s overall usability, and this spiral process continued until consensus was reached amongst all three groups that the model was suitable for integration into learning and assessment.
The simulated model was used in multiple surgical skills training and assessments in year one of Core Surgical Training (CST) in Ireland. Initial user feedback evaluations of the models’ realism, suitability and practicability were favourable. To further evaluate the training model, criterion for face, content and construct validity will be collected from novice and expert groups.
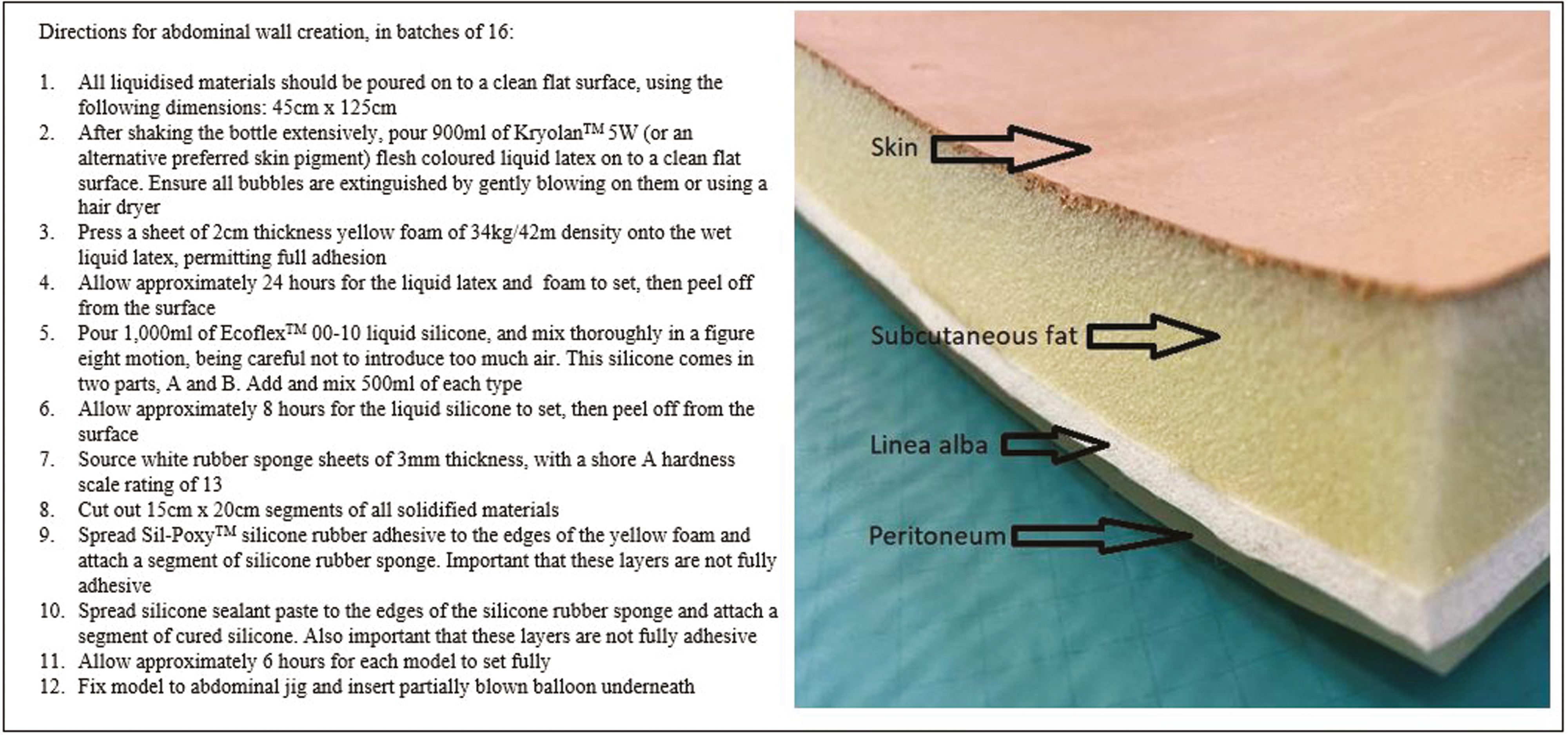
The completed model simulates a midline abdominal incision and closure and integrates the four main tissue layers identified as essential for anatomical representation. The layers are characterized in this model by various synthetic materials (Figure 1). The model is fixed to the surface of a hollow plastic jig of 18-cm depth, with a red balloon inserted within to simulate the viscera and provide depth precision feedback.


The tissue layers are exposed, with two small artery forceps manipulating the peritoneal layer (left). Closure of linea alba using continuous sutures (middle). Closure of skin using staples (right).
Skin is represented by a layer of flesh-coloured liquid latex, providing skin closure opportunities using staples or sutures. The thick subcutaneous fat layer is characterized by yellow foam of low tensile strength. White silicone sponge rubber delineates the fascial layer, with peritoneum illustrated in this model by a thin layer of super soft cured silicone rubber. Super soft silicone allows for creation of thin, firm, elastic sheets, personified in peritoneum. This is of critical importance in terms of safety of abdominal entry, as a thin peritoneal layer allows trainees to demonstrate careful tissue handling. The potential to stray from the midline and penetrate the rectus sheath, especially in obese patients, is a typical issue when creating midline incisions. We recognize this problem as progressing as part of our iterative design process, and efforts will be made to replicate this muscle in future designs.
Each individual model is 15 cm × 20 cm in size, and costs a total of €10.60 for materials. In order to maximize production efficiency in the RCSI SIM innovations lab, models are made in batches of 16. Assembly of each batch takes approximately 60 minutes once all liquidized materials have solidified (see Appendix A for instructions to build the model).
A myriad of similar models are available commercially on the market, and range in price from €18.52 to €87.81 per unit. Our model represents a minimum saving of 42% to that of market equivalents, and its configuration ensures that it is realistic and replicable. Its dimensions ensure that two midline incision and closures can be carried out on each unit, without compromising the models usability.
This model in its current form has the potential for further development, with enhanced representation of the visceral components to allow for advanced skills training. We envision creating a hybrid model, comprising a mixture of biological and synthetic materials, to provide enhanced haptic feedback and to accommodate the use of stapling and energy devices.
Mr. Miroslav Voborsky and Ms. Niamh Murphy from simulation team in RCSI University of Medicine and Health Sciences for their help in creating the abdominal wall model.
None declared
None declared
None declared.
None declared.
None declared.
1.
2.
3.
4.
5.
 Developing a simulation training model for abdominal wall opening and closure
Developing a simulation training model for abdominal wall opening and closure
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets