
Bias potentially affects simulation-based training (SBT) for healthcare professions. The role bias plays in SBT design, presentations, and in the experiences of learners should be understood. Dual process theory is a well-accepted framework for understanding types of bias.
The authors performed a scoping review to map ‘bias’ in SBT of health professions in the literature. Search terms were developed for a query in the PubMed database. Researchers reviewed abstracts, met ten times to discuss which papers’ full texts to read, and then analysed and categorized the articles. Researchers used the Arksey and O’Malley framework for scoping reviews.
Three thousand six hundred and twenty abstracts were identified by a detailed query in the PubMed database of which, 115 full-text articles were identified for inclusion.
Articles published about bias in SBT cover a broad range of topics, from addressing how bias affects patient care, to bias in raters’ scoring of medical students on exams. Researchers found that the prevalence of articles on bias in SBT increased over time and focused primarily on implicit bias. Specific types of bias in some instances were difficult to identify, and several biases mentioned in papers were unique to this review. The results showed that many SBT methodologies (i.e. manikins, videos, etc.) were referenced in the papers. The type of simulation training most prevalent in the articles was simulated patient (SP) methodology. The results show that biases can be explored in any type of simulation method, indicating that simulationsists should be aware of bias in training during all types of training methodolgy.
Simulation-based training (SBT) for healthcare professions is increasingly used as an educational strategy and to improve patient safety [1–4]. SBT is an effective strategy to improve skills in healthcare professions [5]. Many different methodologies have been developed in SBT, and those methodologies have helped achieve learning outcomes, which leads to clinical competency [6]. Patient or human simulation is a well-known methodology involving human role players interacting with health professions’ education in a variety of experiential learning and assessment activities. The term simulated patient (SP) refers to a person trained to portray a role such as patients, clients, family members, healthcare professionals, etc. in realistic and repeatable method. The terms standardized patient and simulated patient are often used synonymously [7].
SBT should be developed and implemented to ensure that clinical competencies including technical, communication, decision-making and team dynamics, etc. are achieved [3]. Because SBT involves decision-making where learners must weigh different options to provide patient care, the role that bias plays in SBT design, presentations and in the experiences of learners should be understood [8].
Scoping reviews are useful when authors want to explore certain concepts in papers, and in the mapping, reporting or discussion of these concepts [9]. There are scoping reviews on SBT of healthcare professions exploring the types of professions engaged in interprofessional education, characterization of the types of simulations, effects of new technologies on SBT, effects of different methodologies on clinical competencies of healthcare professions and barriers to utilization different methodologies [10–12]. We did not find any scoping reviews on the topic of bias in SBT of healthcare professions.
In this review, we sought to explore bias in SBT of healthcare to: 1) identify which types of biases affect SBT for healthcare professionals, 2) categorize the types of bias explored and 3) note the prevalence of articles published on this topic.
We performed a scoping review to map ‘bias’ in the literature on SBT of health professions. Scoping reviews are used to examine the range and nature of the research activities, to determine the value of conducting a complete systematic review, to summarize and disseminate research findings, or to detect gaps in existing literature [13].
We used the Arksey and O’Malley framework for scoping reviews [13] which was developed and refined by Levac and colleagues [14]. This approach involves five steps:
1. Identifying the research question
SA and CP met to identify the focus of the scoping review: ‘How is the term “bias” in “simulation training” explored within the literature?’ After conducting background research, we discovered that the terms ‘cognitive bias’, ‘implicit bias’ and ‘decision-making’ are terms used in conjunction with ‘bias’, therefore it was decided to include these terms along with ‘simulation’ and ‘bias’ in the analysis.
2. Identifying relevant studies
After determining the scoping review goals and receiving assistance from a University of Illinois at Chicago-affiliated librarian, we decided to use a detailed query which included all potential MeSH terms and keywords that might be related to ‘simulation’ and ‘bias’ for a database search (Figure 1).

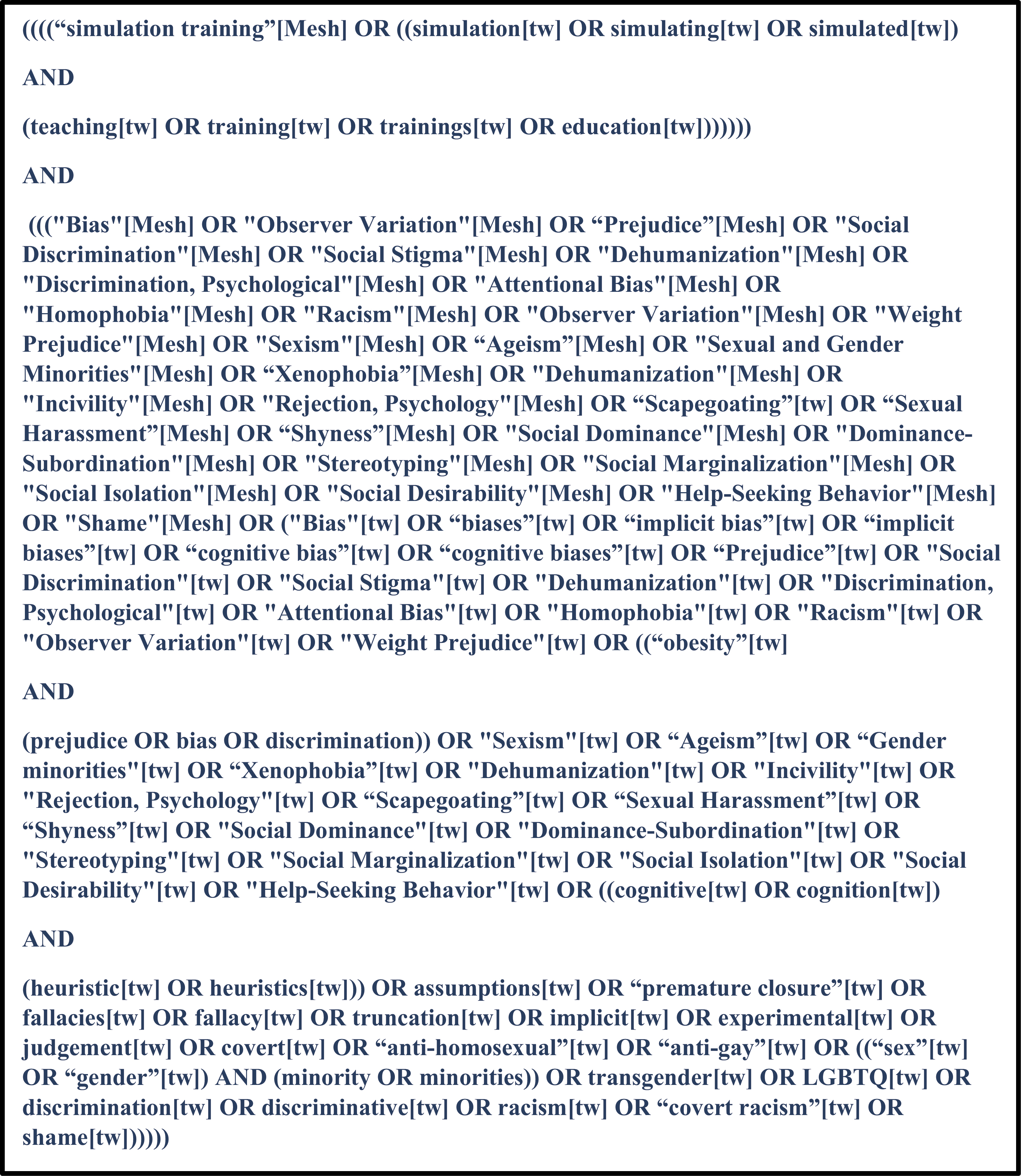
Query for database search.
We searched the PubMed, Medline and CINAHL databases with the same terms, and compared the results. The PubMed results were the most comprehensive and included the results from the other databases, so we decided to focus only on the PubMed database. We limited the results by publication language (English).
3. Selecting the studies
As a first step, researchers SA and ABC conducted a pilot study to determine the method for analyzing the papers for this scoping review. We reviewed the first 100 papers found by a search using the detailed query to determine which articles should be included in the review. We then compared notes on the abstracts and full texts of the papers. We decided to include only primary research articles as it was too difficult to evaluate review papers based on the aims of this scoping review. After this pilot, we decided to select articles for study inclusion based on the following criteria:
(a) studies that investigated bias in simulation training of any health professions’ education program,
(b) studies that investigated the role of bias in simulation training,
(c) original articles, brief reports,
(d) studies in which outcomes/assessment focused on decision-making.
The following exclusion criteria were also defined as:
(a) any type of reviews,
(b) studies written in a language other than English,
(c) studies that did not include any simulation training, and
(d) studies including bias in simulation training, but, without any explanation for bias.
SA and ABC decided to analyze the papers’ abstracts for first reading because it was determined that papers might be selected based on their abstracts (without reading the full text) using the inclusion criteria. SA and ABC independently reviewed all abstracts published up to August 31, 2020. We then discussed any discrepancies and reached a consensus on which articles to include for the full review (second stage of scoping review).
We referred to the papers’ descriptions of the type of bias they addressed, to identify if the bias was implicit or cognitive. In instances where the type of bias was not specified in the paper, we identified the type of bias from the content of the paper, including instances where both cognitive and implicit bias were explored. We then further classified the specific type of bias, again referring to the article’s content. In cases where the bias was the same, but terminology differed between papers (i.e. one paper used the term ‘race bias’, while another referred to is as ‘racial bias’), we standardized the naming of the bias by choosing one term for a similar type of bias.
4. Charting the data
We used Arksey and O’Malley’s ‘descriptive-analysis’ approach to data extraction, summarizing information from the selected articles and recording the data [13]. We also applied Levac and et al.’s recommendations for the data charting process and used an Excel sheet to analyze the selected articles [14]. By using this approach, the key information from the selected papers was charted under the headings: article name, author, journal, year, country, article type, population, details of simulation training and details of bias.
5. Collating, summarizing and reporting the results
Three thousand six hundred and twenty abstracts were identified from PubMed. The first reading was conducted by SA and ABC from May 4, 2020 to August 31, 2020. During this first reading, we met 10 times to discuss which papers should be added for the second step (reading full texts). We reviewed 238 selected papers for the second step, and 125 full-text articles were selected to be analysed from October 23, 2020 to January 12, 2021. We independently read and reviewed the included articles, and reconvened at six online meetings to discuss individual findings (Figure 2).

Results of search strategy and process of paper selection.
From 1985 until 2020, the number of articles published on the topic of bias in simulation in medical professional training increased dramatically (Figure 3).

Classification by year.
We completed a review of articles published on bias in SBT for healthcare professionals. The articles reviewed cover a broad range of topics, from addressing how bias affects patient care, to bias in raters’ scoring of medical students on exams. We did not assess the methodological quality of the articles, but categorized them into four general themes: the type of healthcare profession, the method of simulation, whether the bias was cognitive or implicit, and the specific bias mentioned (Table 1).

| Lead Author | Journal | Year | Country | Population (healthcare professions) | Method(s) of simulation mentioned in article | Bias types | Description of bias |
|---|---|---|---|---|---|---|---|
| Adamson, K. [70] | Nursing education perspectives | 2016 | USA | Simulation participant-raters (nurse) | Video-recorded simulations | Implicit bias | Race, ethnicity bias |
| Al-Moteri, M. [71] | Australian Critical Care | 2019 | Australia | Final-year undergraduate nurses, nurses enrolled in Masters or PhD programs. | Screen-based simulated scenario | Cognitive Bias | Perceptual, attention, confirmation biases |
| Altabbaa, G. [72] | Diagnosis | 2019 | Canada | Medical students, post-graduate year (PGY) 1 IM residents, | Simulated clinical environment | Cognitive Bias | Momentum, confirmation, playing-the-odds, order-effect biases |
| Arber, S. [17] | Social Science & Medicine | 2006 | USA | Primary care doctors | Video vignette | Implicit bias | Gender, age, SES, race biases |
| Barnato, A. [55] | Crit Care Med. | 2011 | USA | Emergency physicians, hospitalists, and intensivists | SPs | Implicit bias | Race bias |
| Barnato, A. [73] | Med Decis Making | 2014 | USA | EM physicians | Video-encounters | Implicit bias | Race bias |
| Bennett, P. [74] | Clin Teach | 2016 | Australia | Medical, nursing, allied health students | Immersive/wearable simulation | Implicit bias | Age bias |
| Berg, K. [18] | Acad Med | 2015 | USA | Medical students | OSCEs | Implicit bias | Gender, race and ethnicity biases |
| Boada, L. [19] | Comput Methods Programs Biomed | 2018 | Spain | Undergraduate nursing students | High fidelity simulators | Implicit bias | Gender bias |
| Bond, W. [75] | Acad Med | 2004 | USA | Emergency medicine residents | High fidelity simulators | Cognitive bias | Decision-making |
| Boulet, J. [20] | Adv Health Sci Educ Theory Pract | 2005 | USA | Medical students (CSA candidates)/physician note raters | SPs | Implicit and Cognitive Biases | Gender and rater bias |
| Braun, L. [76] | Diagnosis | 2019 | Germany | Medical students | Electronic case simulation platform | Cognitive Bias | Premature closure bias |
| Brown, S. [77] | Community Ment Health J | 2010 | USA | Undergraduate medical students | Simulation of auditory hallucinations | Implicit bias | Illness stigma |
| Brown, SA. [78] | Community Ment Health J | 2010 | USA | Undergraduate students | Simulation of auditory hallucinations | Implicit bias | Mental illness stigma |
| Bucknall, T. [79] | J Adv Nurs | 2016 | Australia | Nursing students (final year) | SPs | Cognitive bias | Premature closure and confirmation biases |
| Burgess, D. [80] | Soc Sci Med | 2008 | USA | Internal medicine physicians | Video vignettes | Implicit bias | Race bias |
| Cavalcanti, R. [56] | Acad Med | 2014 | Canada | Residents in internal medicine | OSCEs and High fidelity simulators | Cognitive bias | Not specified |
| Chen, A. [81] | Am J Pharm Educ | 2011 | USA | Pharmacy students | Geriatric medication game and SPs | Implicit bias | Age bias |
| Choi, H. [82] | Nurse Educ Today | 2016 | Korea | Undergraduate nursing students | SPs | Implicit bias | Mental illness stigma |
| Chugh, U. [83] | Med Teach | 1993 | Canada | Physicians/immigrant patients | SPs | Implicit bias | Race and Ethnicity bias |
| Cicero, M. [84] | Prehosp Emerg Care | 2014 | USA | SPs, high-fidelity manikins, and low-fidelity manikins | Disaster simulation scenarios using SPs, high-fidelity manikins, and low-fidelity manikins | Cognitive bias | Bias towards a specific pediatric disaster triage strategy |
| Claramita, M. [85] | Nurse Educ Today | 2016 | Indonesia | Nursing students | OSCE with SPs | Cognitive bias | SES bias |
| Clark, C.M. [86] | Nurse Educ | 2019 | USA | Undergraduate nursing students | Role play | Implicit bias | Uncivil behavior bias |
| Crapanzano, K. [87] | J Gen Intern Med | 2018 | USA | Internal medicine residents | SPs | Implicit bias | Mental illness stigma |
| Dearing, K. [88] | J Nurs Educ | 2008 | USA | Nursing students | Voice simulation mimics auditory hallucinations | Implicit bias | Mental illness stigma |
| Dedy, N. [45] | Surgery | 2015 | Canada | Surgery residents | OSCE | Implicit bias | Rater bias |
| Denney, M. [21] | Educ Prim Care | 2016 | UK | GPs | OSCE | Implicit bias | Ethnicity and gender bias |
| Doyle, K. [46] | J Grad Med Educ | 2014 | Canada | Faculties and residents of family medicine programs | Simulated a tri-college, on-site ER for internal review (IR) process | Implicit bias | Rater/reviewer bias |
| Eisenberg, E. [22] | J Gen Intern Med | 2019 | USA | First-year residents in the Internal Med-Residency Program | Simulation scenarios included interactions with SPs | Implicit bias | Race, ethnicity, nationality, religion, gender, sexual orientation, disability, physical appearance, SES biases |
| Eva, K. [89] | Acad Med | 2010 | Canada | Primary care physicians | Videotaped vignette | Cognitive bias | Confirmation, and premature closure bias |
| Evans. J. [90] | Issues Ment Health Nurs | 2015 | Australia | 2nd year nursing students | Simulated auditory hallucinations for schizophrenics | Implicit bias | Mental illness stigma |
| Feldman, H. [23] | Health Serv Res | 1997 | USA | Physicians | Simulated scenarios on videotapes by professional actors | Implicit bias | Age, gender, race, and SES biases |
| Fitzgerald, S. [91] | MedEdPORTAL | 2018 | USA | Health professions students from multiple disciplines | SPs | Implicit bias | Ethnicity bias |
| Fletcher, G. [47] | Br J Anaesth | 2003 | UK | Anesthetists | SPs | Cognitive bias | Rater bias |
| Floyd, K. [92] | J Physician Assist Educ | 2015 | USA | Physician assistant students/2nd yr of MS degree and SPs | SPs | Cognitive bias | Inflation bias |
| Foster, K. [93] | Oral Surg Oral Med Oral Pathol Oral Radiol Endod | 2008 | USA | 1st year dental students | Role play practice | Cognitive bias | Presentation bias |
| Galletly, C. [94] | Aust N Z J Psychiatry | 2011 | Australia/New Zealand | Medical students (final year) | Video presentation/Simulated auditory hallucinations | Implicit bias | Mental illness stigma |
| Gispert, R. [24] | Med Educ | 1999 | Spain | Undergraduate medical students | SPs | Implicit bias | Gender bias |
| Goddard, L. [95] | J Neurosci Nurs | 1998 | USA | Nursing students | Role play | Implicit bias | Disability bias |
| Gostlow, H. [96] | Ann Surg | 2018 | Australia | Surgical trainees and consultant surgeons | Video of operating theater sim – SPs | Implicit bias | Hierarchy bias |
| Gotlieb, R. [97] | Gynecologic Oncology Reports | 2019 | Canada | Medical doctors (staffs and residents) | Software (computer) simulation scenarios. | Cognitive Bias | Gender effects on cognition |
| Greene, R.E. [25] | Med Educ | 2014 | USA | Medicine residents | SPs | Implicit bias | Gender bias |
| Greene, R.E. [26] | J Grad Med Educ | 2017 | USA | Medicine students | SPs | Implicit bias | Gender bias |
| Hahn, T. [98] | J Man Manip Ther | 2014 | USA | Physical therapists | Video vignettes of SPs | Cognitive bias | Confirmation bias/ and training bias |
| Hales, C. [99] | Ostomy Wound Manage | 2018 | USA | Health care staff | Immersive/wearable simulation | Implicit bias | Weight bias |
| Haliko, S. [100] | Med Decis Making | 2018 | USA | Physicians | High fidelity simulator and SPs | Cognitive bias | Preference and comfort bias |
| Hanson, M. [101] | Acad Psychiatry | 2008 | Canada | Adolescent standardized patients | SPs | Implicit bias | Mental illness stigma |
| Hareli, S. [102] | Int J Psychol | 2013 | Israel | Undergraduate medical students | Video on computer screen simulation | Implicit bias | SES bias |
| Hermann-Werner, A. [103] | BMJ Open | 2019 | Germany | Medical students | SPs and immersive/wearable simulation | Cognitive Bias | Weight bias |
| Hillbrand, M. [104] | Psychiatr Rehabil | 2008 | USA | Nurses, psychiatric technicians, psychologists and social workers, rehabilitation therapist. | Role play | Implicit bias | Bias against prisoners |
| Hirsh, A. [27] | J Pain | 2010 | USA | Nurses | Virtual human (VH) videos | Implicit bias | Gender, race, age bias |
| Hu, Y. [105] | Adv Health Sci Educ Theory Pract | 2015 | USA | Undergraduate medical students | Simulation-based suturing task | Cognitive bias | Overestimation bias |
| Huber, M. [106] | J Adv Nurs | 1992 | USA | Healthcare care personnel | Simulated handicaps | Implicit bias | Age bias |
| Hunter, J. [107] | Nurse Educ Today | 2018 | UK | Nursing Students | Immersive/wearable simulation | Implicit bias | Weight bias |
| Jaeken, M. [108] | Front Psychol | 2017 | Belgium | Undergraduate psychology students | Role play | Cognitive bias | Self-enhancement bias |
| Jaworsky, D. [109] | AIDS Care | 2017 | Canada | Medical Students | SPs | Implicit bias | HIV stigma |
| Jensen, K. [48] | Surg Endosc | 2019 | Multi-centered | Medical students | Virtual reality simulator | Cognitive bias | Self-enhancement and self-diminishment bias |
| Junnola, T. [110] | J Clin Nurs | 2002 | Finland | Nurses | Screen-based computer simulated case | Cognitive bias | Confirmation bias |
| Kales, H. [28] | Psychiatr Serv | 2005 | USA | Psychiatrists | Video vignettes of SPs | Implicit bias | Race and gender bias |
| Kennedy, D. [29] | Nurse Educ Today | 2020 | Qatar | Male nursing students | Role-play, moderate and high fidelity simulators, SPs, simulated maternity clinic | Implicit bias | Gender bias |
| Khazadian-Figueroa, M. [111] | J Nurs Staff Dev | 1997 | USA | CNAs (certified nursing aids) | Simulation game | Implicit bias | Age bias |
| Kidd, L. [112] | Issues Ment Health Nurs | 2015 | USA | Undergraduate psychiatric nursing students | Hearing Distressing Voices Audio Simulation | Implicit bias | Mental illness stigma |
| Kim, M. [30] | Comput Inform Nurs | 2016 | Korea | Nursing students | Simulation-based learning/hybrid SP and Noelle human simulator | Implicit bias | Gender bias |
| Kumagai, A. [31] | Med Teach | 2007 | USA | Faculty | ‘Forum Theater’ techniques; simulated classroom discussion | Implicit bias | Race, gender, sexual orientation, SES bias |
| Kushner, R. [113] | BMC Med Educ | 2014 | USA | Medical students | SPs | Implicit bias | Weight bias |
| LaRoche, K. [114] | Contraception | 2015 | Canada | Postabortion support team | Unannounced standardized patient | Implicit bias | Abortion stigma |
| Levett-Jones. T. [115] | Nurse Educ Pract | 2011 | Australia | Nursing Students | Videos w/SPs to train assessors | Implicit and Cognitive biases | Rater/Assessor bias Decision-making |
| Lewis, C. [116] | BMC Palliat Care | 2016 | UK | Nursing and medical students | High fidelity simlulator and SP | Implicit bias | Attitudes towards death |
| Li, L. [117] | Int J Epidemiol | 2014 | China | Hospital service providers | Unannounced standardized patient | Implicit bias | HIV stigma |
| Lockeman, K.S. [118] | Nurse Educ Today | 2017 | USA | Nursing and medical students | high fidelity – mannequins and SPs | Implicit Bias | Provider stereotypes |
| Lohman, P. [119] | Percept Mot Skills | 2008 | USA | Graduate students majoring in communications disorders | Peer role play | Implicit bias | Attitudes towards stutterers |
| Lorenzo, A. [120] | Fam Pract | 2015 | France | Practicing providers | SPs | Cognitive bias | Desirability bias/Hawthorne bias |
| Magpantay-Monroe, E. [121] | Nurse Educ Today | 2017 | USA | Nursing students | SPs | Implicit bias | Military and veteran bias |
| Marceau, L. [32] | J Eval Clin Pract | 2011 | USA | Primary care physicians | Video simulation | Implicit bias | Age, race, gender, SES biases |
| March, C. [122] | J Grad Med Educ | 2018 | USA | Pediatric residents | SPs | Implicit bias | Age, race and ethnicity stigma |
| Margolis, M. [33] | Acad Med | 2002 | USA | Medical doctors | Computer-based case simulation | Implicit bias | Gender and language bias |
| Maruca, A.T. [123] | Nurse Educ Perspect | 2018 | USA | Nursing students | High fidelity (manikin) simulation | Implicit bias | Gender bias |
| Maupome, G. [124] | Eur J Dent Educ | 2002 | Mexico | Senior dental students | SPs | Implicit bias | SES bias |
| McCave, E. [34] | MedEdPORTAL | 2019 | USA | Students’ of different health professions | SPs | Implicit bias | Gender bias |
| McGrath, J. [49] | West J Emerg Med | 2015 | USA | EM residents | High fidelity and virtual reality simulators | Implicit bias | Rater/observer bias |
| McNiel, P.L. [35] | J Nurse Educ | 2018 | USA | Nursing students | Role play | Implicit bias | Gender biases |
| Minehart, R. [125] | Anesthesiology | 2014 | USA | Anesthesia faculty | Role play/videos/SPs | Cognitive bias | Not specified |
| Mirza, A. [126] | MedEdPORTAL | 2018 | USA | Pediatric interns, upper-level residents (PGY-2 and PGY-3), and six fellows. | SPs | Cognitive Bias | Premature closure bias |
| Mohan, D. [127] | BMC Emerg Med | 2016 | USA | Emergency physicians | Virtual video games simulation | Cognitive bias | Poorly-calibrated heuristics |
| Nerup, N. [50] | Gastrointest Endosc | 2015 | Denmark | Physicians (10 experienced endoscopists and 11 trainees) | High fidelity simulator | Implicit bias | Rater/observer bias |
| Nicolai, J. [36] | Patient Educ Couns | 2007 | Germany | General practitioners | SPs | Implicit bias | Gender bias |
| Norman, R. [128] | J Nurs Educ | 2001 | Australia | RNs (nurses) | Simulation game, peer role playing | Implicit bias | Bias against illicit drug users |
| O’Lynn, C. [129] | J Nurse Educ | 2014 | USA | Male nursing students | Video and practice on manikins/debriefing | Implicit bias | Gender bias |
| Padilha, J. [57] | J Med Internet Res | 2019 | Portugal | Nursing students | Virtual reality simulator | Cognitive bias | Bias in clinical reasoning |
| Paige, J. [130] | J Surg Educ | 2019 | USA | General surgery residents/ emergency medicine residents/senior undergraduate nursing students | High fidelity simulation | Implicit bias | Hierarchy bias |
| Park, C. [58] | Simul Healthc | 2014 | USA | Residents, Anesthesiology (PG2) | Simulated operating room/simulated scenario | Cognitive bias | Not specified |
| Patterson, F. [131] | Med Educ | 2018 | UK | Medical students | High fidelity simulator | Implicit bias | Ethnicity bias |
| Pennaforte, T. [132] | JMIR Res Protoc | 2016 | Canada | General Pediatrics and Neonatal-Perinatal Medicine residents. | Simulation scenario and standardized health professionals | Cognitive bias | Not specified |
| Persky, S. [133] | Ann Behav Med | 2011 | USA | Undergraduate medical students | Immersive virtual environment/computer generated | Implicit bias | Weight bias |
| Prakash, S. [134] | BMC Med Educ | 2017 | Australia | Interns (medical students) | High-fidelity simulator and SPs | Cognitive bias | Search satisfying, premature closure, and anchoring bias |
| Raemer, D.B. [37] | Acad Med | 2016 | USA | Anesthesiologist | Simulated scenarios | Implicit bias | Hierarchy, gender and stereotypes bias |
| Richey Smith, C. [135] | Am J Pharm Educ | 2016 | USA | Pharmacy students | Simulation game | Implicit bias | SES bias |
| Richmond, A. [136] | MedEdPORTAL | 2017 | USA | Students/medicine, nurse, pharmacy | SPs | Implicit bias | Hierarchy bias |
| Ruparel, R. [137] | J Surg Educ | 2014 | USA | 27 urology residents | Virtual reality simulator | Cognitive | Internal bias (experience w/simulator not translating to surgery affecting confidence) |
| Rutledge, C. [138] | Contemp Nurse | 2008 | USA | Nurses | Computer generated virtual learning platform, high performance simulators (HPS). | Implicit bias | Cultural bias |
| Sargeant, S. [38] | Adv Health Sci Educ Theory Pract | 2017 | Australia | Medical students/SPs | SPs | Implicit bias | Culture, age, gender biases |
| Schuler, S. [139] | Stud Fam Plann | 1985 | USA/Nepal | Family planning staff | SPs | Implicit bias | Hierarchy bias |
| Sidi, A. [140] | J Patient Saf | 2017 | USA | Residents | High fidelity simulator | Cognitive bias | Anchoring, availability bias, premature closer and confirmation bias |
| Siegelman, J.N. [39] | J Grad Med Educ | 2018 | USA | Emergency medicine residents | Simulated cases – SPs, nurses, and simulation operators | Implicit bias | Gender bias |
| Silverman, A.M. [141] | Disabil Rehabil | 2018 | USA | Masters of occupational therapy (1st year) | Impairment simulation (role play) | Implicit bias | Anti-disability and discriminatory bias |
| Stockmann, C. [40] | J Nurse Educ | 2017 | USA | Nursing students | Manikin | Implicit bias | Gender bias |
| Svendsen, M. [51] | World J Gastrointest Endosc | 2014 | Denmark | Ten consultants experienced in endoscopy (gastroenterologists, n = 2; colorectal surgeons, n = 8) and eleven fellows | Virtual reality simulator | Implicit and Cognitive biases | Rater/observer bias Decision-making |
| Theodossiades, J. [142] | Ophthalmic Physiol Opt | 2012 | UK | Optometrists | Unannounced standardized patients | Cognitive | Self-reporting bias |
| Thompson, C. [143] | J Adv Nurs | 2012 | UK | Nursing students, nurses | Low and high fidelity/paper cases and human simulation (manikins not actors) | Cognitive | Judgment bias |
| Tollison, A.C. [41] | J Nurse Educ | 2018 | USA | Male nursing students | Online simulation | Implicit bias | Gender bias |
| Underman, K. [42] | MedEdPORTAL | 2016 | USA | Undergraduate medical students | SPs | Implicit bias | Gender bias |
| Varas-Diaz, N. [144] | J Gay Lesbian Soc Serv | 2019 | USA | Physicians in training | SPs | Implicit bias | Gender and sexual orientation bias |
| Watson, M. C. [145] | Pharm World Sci | 2004 | UK | Emergency medicine residents | Simulation lab scenario/high fidelity simulation | Cognitive bias | Selection bias |
| Welch, L. [43] | J Health Sco Behav | 2012 | UK | Primary care physicians | Video vignettes of SPs | Implicit bias | Gender bias |
| Wijnen-Meijer, M. [52] | Adv Health Sci Educ Theory Pract | 2013 | Netherlands/Germany | Physicians | SPs | Cognitive bias | Rater bias Decision-making |
| Wiskin, C. [44] | Med Educ | 2004 | UK | Medical students | Role-play | Implicit bias | Gender bias |
| Woda, A. [146] | Nurs Educ Perspect | 2019 | USA | Nursing students | Simulated clinical environment | Cognitive bias | Bias in clinical reasoning |
| Worth-Dickstein, H. [147] | Teach Learn Med | 2005 | USA | Medical Students | SPs | Implicit bias | SP scoring, personal, race, ethnic, and age bias |
| Wu, B. [148] | BMC Med Educ | 2016 | Hong Kong | Medical students | Simulated cases – cognitive mapping | Cognitive bias | Bias in clinical reasoning |
| Yeates, P. [149] | BMC Med | 2017 | UK | Undergraduate medical students | SPs | Implicit bias and Cognitive bias | Race, ethnicity, and examiner, recollection bias |
| Yu, C. [150] | J Am Geriatr Soc | 2012 | Taiwan | Nursing assistants | SPs | Implicit bias | Age bias |
| Yuan, M. [151] | Interact J Med Res | 2013 | USA | Nurse evaluators | SPs | Cognitive bias | Premature closure, anchoring, confirmation, and framing bias |
| Yudkowsky, R. [152] | Acad Med | 2015 | USA | Medical students | SPs | Cognitive bias | Confirmation bias |
| Yule, S. [153] | World J Surg | 2008 | Scotland | Surgeons | Videos of SPs and High fidelity simulator | Cognitive bias | Competency bias |
| Zottmann, J.M. [154] | GMS J Med Educ | 2018 | Germany | Medical students | High fidelity simulator | Cognitive bias | Competency bias |
Dual process theory is a well-accepted framework for understanding decision-making processes and bias. This theory explains our thinking processes as either type 1 or type 2. Type 1 thinking is a fast, intuitive, pattern recognition-focused problem-solving method that creates a low cognitive burden on the user and enables quick decisions. Type 2 thinking is a slower, more methodical, thoughtful process. Therefore, an optimal balance of type 1 and type 2 processes is required to prevent biases for optimal clinical practice [15].
In dual process theory, type 2 thinking can bring a higher cognitive strain on the user but allows them to evaluate data more critically and look beyond patterns, and may potentially be more appropriate for complex problem solving. The current opinion among psychologists is that we spend approximately 95% of our time in type 1 thinking [16]. Cognitive bias (and the resulting errors) are more likely during the type 1 process [15].
Optimal diagnostic approaches are likely to use both type 1 and type 2 thinking at appropriate times. Non-analytical (type 1) reasoning has been shown to be just as effective as reflective reasoning to diagnose routine clinical cases. Furthermore, not all biases are caused by type 1 processing, but it is believed that when bias occurs, it can only be solved by activating type 2 processing. The articles we reviewed showed that the biases explored in articles on SBT were related to both cognitive and implicit biases, both of which can be associated with the two types of dual theory.
In this scoping review, we looked for all types of cognitive and implicit biases in SBT of health professions. Implicit biases were explored more than cognitive biases (Figure 5). The most researched implicit bias in health professions’ SBT is ‘gender bias’ [17–44]. Gender bias was also explored in different types of health professions and with different levels of experience: residents, primary care physicians, medical students, nursing students, etc. The most researched cognitive bias in literature is ‘decision-making (premature closure)’ [20,45–52]. We noted some biases that were not found in other reviews: uncivil behavior bias; poorly calibrated heuristics; and selection bias of patient participants [53–56]. In several papers, the type of bias was not specified and in those instances, we classified the biases based on the article’s content [20,47,51,52]. We were unable to further classify the types of bias explored in a couple of papers [57,58]. Our review indicates the prevalence of undefined bias in simulation training, which supports the importance of educators’ awareness of bias. All biases explored were classified under cognitive and implicit biases.

Types of biases.

Simulation training methods.
Cognitive bias is defined as unconscious and automatically developed mental processing strategies. These strategies are developed as adaptive mechanisms to simplify the complex inflow of information ultimately leading to biased judgments and inferences [59].
Cognitive bias and its impact are an important parameter on decision-making processes [60,61]. Cognitive bias, also known as ‘heuristics’, are cognitive shortcuts to help us make decisions [62]. It is increasingly accepted that significant diagnostic error can result from cognitive bias [63]. Clinical decision-makers have a risk of error due to biases that are not associated with intelligence or any other measure of cognitive ability [64]. In addition, individuals lack awareness of how these biases can affect their perceptions as they are unaware that their judgments are biased. The doctors who describe themselves as ‘excellent’ decision-makers and ‘free from bias’, often lack insight into their own bias [65].
We explored papers on the effects of different simulation methodologies on clinical reasoning and decision-making, and we explored which types of biases affect clinical reasoning and decision-making in SBT.
The natural tendency of the mind is to rely on type 1 thinking, interpret data through heuristic scanning, and establish quick connections with data and experiences already available. Beyond cognitive bias, which affects clinicians’ interpretation of clinical data, there are intuitive screening and systematic biases on how we perceive other people, including patients. The ways we perceive and classify other individuals based on their characteristics (i.e. social and cultural biases) are most likely shaped by the experiences we have been exposed to. In clinicians, these biases appear in parallel with the general population [66]. Implicit bias (sometimes called unconscious bias) affects interpersonal interactions in ways that we are not consciously aware of. The health and behavioral effects of these implicit attitudes can be important. Implicit bias has many dimensions. Some examples of implicit biases are: race or ethnicity, gender, age, weight, sexual orientation, education and socioeconomic status [67].
Meanwhile, experimental studies have repeatedly shown that these biases measurably affect clinical assessments and treatment decision-making [68]. This effect seems particularly significant in challenging or ambiguous situations, or under heavier cognitive loads.
In addition, we noted that the number of articles published on the topic of bias in simulation in healthcare professional training increased dramatically from 1985 until 2020. This increase could reflect the increasing attention paid to decision-making processes and bias in general. It could also be a snowball effect – the more papers published on a topic, the more authors become inspired to explore new data on biases in SBT.
Biases were explored using different simulation methods (Figure 4). Most of the articles exploring biases in simulation training involved SP methodology. This may reflect the importance of SP methodology as a training approach, its prevalence, or the particular need for well-designed scenarios in SP methodology. While SP methodology was the modality most often referred to in the articles, other modalities were also present (i.e. manikins, videos, etc.)
All trainings can be subject to bias. SBT has enhanced learning, however, trainers and learners can benefit from understanding that biases might be present in SBT [58,69]. The results also show that biases can be explored in any type of training methods in simulation, indicating that simulationsists should be aware of bias in training during all types of training.
One limitation of our review is that we only reviewed articles available in English. Additionally, there is no comprehensive classification guide for biases, especially implicit biases, so, we had some difficulties defining or naming some types of bias mentioned in the papers.
Another limitation is that we only reviewed articles found in one database, it is possible that some articles on bias in simulation training of healthcare professionals are included in a database other than PubMed. We also focused on peer-reviewed literature and therefore did not include literature produced outside of traditional academic publishing.
Understanding how bias affects SBT for healthcare professionals is important, as it affects not only how future providers are educated and develop their clinical decision-making skills, but also because of its impact on patient care and health outcomes. This review not only showed the depth of the types of bias examined in the literature, but also found some biases that had not been previously classified.
In future, researchers might explore how biases affect clinical reasoning and decision-making in SBT. Researchers might also explore how to avoid bias in simulation by looking at instructional design of SBT.
There are many opportunities for researchers to explore bias and its impact on SBT. Once SBT trainers become aware of the possible presence of bias in their methodology, they may adjust existing instructional design, better follow established best practices and create new best practices to help identify and address these biases.
We acknowledge and thank Maureen Clark, Librarian at University of Illinois Chicago for her assistance in developing the search terms for this scoping review.
Selçuk Akturan, MD, Christine Park, MD, and Amy Binns-Calvey all made substantial contributions to the conception or design of the work as well as acquisition and analysis of the data. All authors contributed to and provided final approval of the manuscript to be published and are accountable for the accuracy and integrity of the manuscript.
None to declare.
Availability of data and materials: The datasets analyzed during the current review are available from the corresponding author on reasonable request.
This research does not contain any human subjects.
The authors declare that they have no conflict of interest.
None declared.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
93.
94.
95.
96.
97.
98.
99.
100.
101.
102.
103.
104.
105.
106.
107.
108.
109.
110.
111.
112.
113.
114.
115.
116.
117.
118.
119.
120.
121.
122.
123.
124.
125.
126.
127.
128.
129.
130.
131.
132.
133.
134.
135.
136.
137.
138.
139.
140.
141.
142.
143.
144.
145.
146.
147.
148.
149.
150.
151.
152.
153.
154.
 Bias in simulation training for healthcare professions: a scoping review
Bias in simulation training for healthcare professions: a scoping review
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets